Pain in the Head and Neck Is Rarely Simple
Pain in the head and neck does not behave the way most patients — or many providers — expect it to. It refers. It overlaps. It appears in one location while originating in another. A patient with severe facial pressure may not have a sinus problem at all. A patient with chronic ear fullness may have nothing wrong with their ear. A patient with persistent throat irritation may have a problem that begins in the stomach and travels upward silently overnight. In thirty years of rhinologic practice, the single most common clinical error I encounter is the assumption that where pain is felt is where pain is coming from.
This piece is about a framework — one I have refined through decades of clinical work — for approaching pain in the ENT anatomical territory with enough precision to identify its real driver and match treatment to that driver rather than to the symptom alone. The framework is not complex. But it requires a willingness to ask a different question than the one most urgent care visits, primary care appointments, and even some specialist consultations ever get around to asking.
The Biggest Misconception: Pain Does Not Equal Infection
If I could change one thing about how head and neck pain is approached across the healthcare system, it would be the reflexive equation of facial pain and pressure with bacterial sinusitis requiring an antibiotic. This equation is wrong in the majority of cases where it is applied. Pain in the sinuses, face, and head is most commonly driven by inflammation, pressure dysregulation, or nerve irritation — not infection. The 2025 AAO-HNS Clinical Practice Guideline on Adult Sinusitis makes this explicit: watchful waiting without antibiotics is now the recommended approach for most presentations of acute rhinosinusitis, and chronic rhinosinusitis is defined as a primarily inflammatory rather than primarily infectious disease.1
When patients come to me after four or five antibiotic courses for sinus pain, their sinus cultures — when finally obtained — often show organisms that the prescribed antibiotics were never capable of reaching, embedded in biofilm structures that oral antibiotics cannot penetrate at clinical concentrations.2 The pain was not caused by an infection. The antibiotic did not resolve the pain. And yet the prescription cycle continues because the question “what system is actually driving this?” was never asked.
The Three-Bucket Framework
When a patient asks me what is causing their pain, I organize my thinking into three buckets before I say anything else. Not because the answer will always fit neatly into one of them — it usually does not — but because the framework prevents me from anchoring prematurely on the most obvious explanation and missing the actual driver.
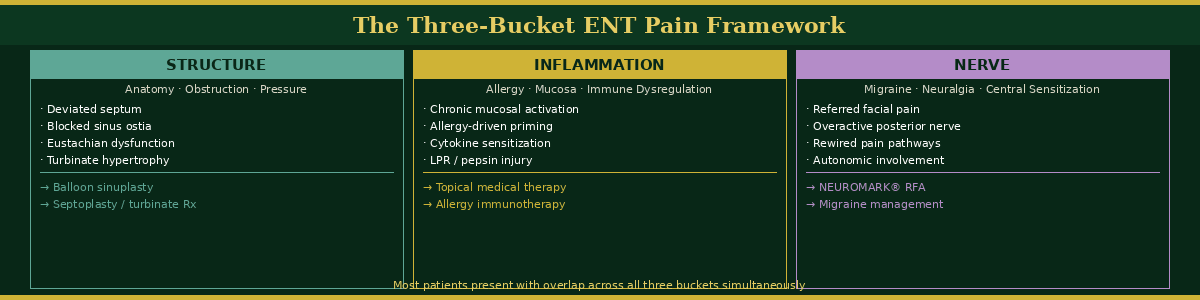
The first bucket is Structure: anatomy, obstruction, and CT findings. The second bucket is Inflammation: allergy, mucosal disease, and immune dysregulation. The third bucket is Nerve: migraine pathways, peripheral neuralgia, and central sensitization. Most patients with significant ENT pain have contributions from more than one bucket simultaneously, and the clinical question is not which bucket applies but rather how much each one is contributing and which driver needs to be addressed first.
The three-bucket framework: mapping ENT pain to its structural, inflammatory, or neurological driver — most patients present with overlap across all three.
When I tell a patient “we are going to map the problem, not guess,” I mean this literally. We are going to use endoscopy to look at the anatomy in real time. We are going to use CT imaging when appropriate to characterize the structural and mucosal picture. We are going to take an allergy history and consider testing. We are going to ask about migraine, about jaw clenching, about neck tension, about reflux, about sleep quality. All of those inputs feed into the three-bucket framework and together they produce a clinical map that guides treatment selection. A map is not a guess. Patients respond differently to a clinician who has a map. The uncertainty does not go away — but the plan becomes visible, and visible plans reduce fear.
“The framework below maps the three primary drivers of ENT pain — Structure, Inflammation, and Nerve — and the treatment modalities that correspond to each. Most patients present with overlap across all three buckets simultaneously, which is why single-intervention approaches so consistently fail.”
Structural Pain — When Anatomy Is the Driver
Structural pain in the ENT anatomical territory is driven by obstruction, pressure dysregulation, and anatomical mismatch between the mucosal volume the system is trying to drain and the aperture it is trying to drain through. A severely deviated nasal septum does not simply obstruct breathing — it creates turbulent airflow, mucosal contact points, and pressure differentials that generate referred facial pain, headache, and ear fullness that a patient may have been told for years is migraine, TMJ dysfunction, or stress. A blocked sinus ostium builds pressure that patients describe as a vice grip behind the eye or a weight across the cheekbones. An Eustachian tube that cannot equalize pressure generates ear fullness, clicking, and pain that feels entirely like an ear problem but originates entirely in the nasopharynx.
Structural pain responds to structural intervention. Balloon sinuplasty restores ostial patency without mucosal resection, allowing the pressure gradient across the blocked sinus to normalize and the pain driven by that gradient to resolve.3 Septoplasty eliminates the contact points and turbulent flow dynamics that drive structural facial pain. Eustachian tube dilation addresses the nasopharyngeal pressure dysregulation driving apparent ear pain. In each case, the procedure is matched to the structural driver — not to the symptom location where the patient experiences the pain.
Inflammatory Pain — The Mucosal Signal
Inflammatory pain is the most commonly missed category in primary care ENT management because it does not always produce findings on CT imaging, it does not always respond to antibiotics, and it does not always have an obvious allergic trigger that the patient can name. The mucosal inflammatory state — driven by allergy, environmental exposure, immune dysregulation, or pepsin-driven posterior nasal mucosal injury in patients with silent laryngopharyngeal reflux — creates a chronic low-grade activation of the sinonasal pain signaling network that patients experience as persistent facial pressure, heaviness, post-nasal irritation, and congestion that never fully resolves between episodes.
This is the patient who keeps returning to urgent care. Their CT is normal or minimally abnormal. Their cultures are negative. Their antibiotics help for two weeks and then the symptoms return. What they have is not an infection. They have a chronically inflamed mucosal system that is generating a continuous pain signal through cytokine-driven sensitization of the trigeminal branches innervating the sinonasal mucosa.4 Treating this with an antibiotic is treating the wrong bucket. Treating it with topical corticosteroids, allergy management, nasal saline irrigation, and — in the appropriate patient — pepsin-directed medical management addresses the actual inflammatory driver. The pain resolves not because the infection was treated but because the inflammatory state was.
Acute Versus Chronic Pain — Two Completely Different Systems
One of the most important conversations I have with patients is the distinction between acute and chronic pain — because they are not the same physiological phenomenon, and treating chronic pain as if it were simply prolonged acute pain produces consistently poor outcomes.
Acute pain is an alarm system. Something new has occurred. The signal is roughly proportional to the degree of tissue damage or threat. It is designed to be temporary, and as healing progresses, the signal diminishes. In the ENT context: an acute sinus infection produces acute pain. The infection resolves, the inflammation resolves, and the pain resolves with it. This is the alarm doing exactly what it is designed to do.
Acute pain signals a new problem in a functional system. Chronic pain reflects a rewired system — requiring a reset, not simply removal of disease.
“The distinction between acute and chronic pain is not simply a matter of duration — it reflects two fundamentally different physiological states requiring completely different treatment philosophies. Understanding which system a patient is in changes everything about how healing is approached and how long it realistically takes.”
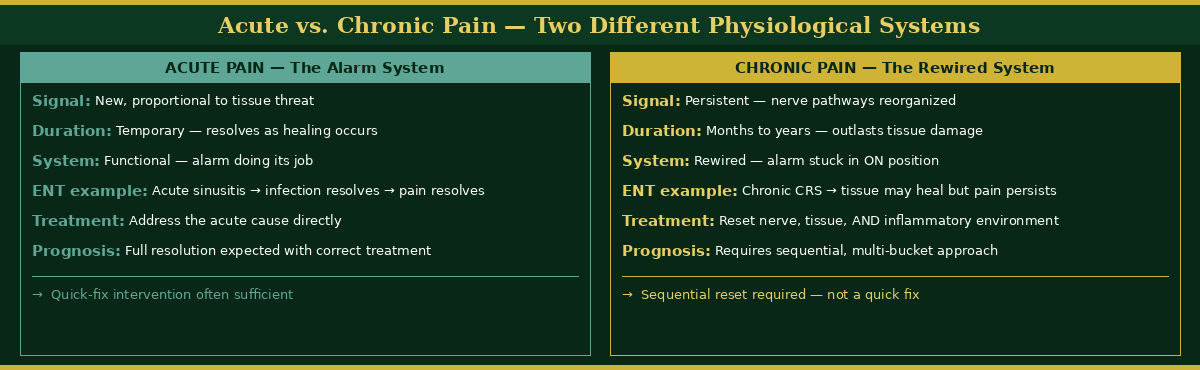
Chronic pain is a rewired system. The signal has persisted long enough that the nerve pathways themselves have reorganized. Central sensitization has developed — the brain’s pain processing centers have been recalibrated to interpret signals as painful that would not previously have reached conscious awareness. The tissue damage may have resolved or never been significant in the first place, but the pain persists because the system that was supposed to generate the alarm has become stuck in the alarm state. In chronic ENT conditions — chronic rhinosinusitis, refractory post-nasal drainage, persistent facial pressure of years’ duration — healing means not simply removing the disease but resetting the tissue, the nerve pathways, and the inflammatory environment that has sustained the rewired state. This takes time. It requires patience from both the patient and the clinician. And it requires a treatment plan that addresses the full system rather than just the most visible component of it.
The Physical-Psychological Integration
Pain is often described in clinical contexts as either physical or psychological — a distinction that implies they are different categories of experience with different clinical validity. I do not accept this distinction, and neither does the neuroscience of pain.5 The airway is deeply connected to the autonomic nervous system, the stress response, and the inflammatory signaling network simultaneously. Emotional stress activates the hypothalamic-pituitary-adrenal axis, elevates cortisol, increases systemic inflammatory tone, and directly amplifies the mucosal inflammatory state driving sinonasal pain. Physical inflammation — chronic sinonasal inflammation in particular — drives central sensitization, disrupts sleep architecture, impairs cognitive function, and contributes to mood dysregulation through the same cytokine pathways that are driving the nasal symptoms.
This is one connected system. Patients who feel dismissed when their imaging does not match their symptom severity are often experiencing the clinical consequence of central sensitization — their nervous system has been recalibrated by months or years of chronic inflammatory signaling to the point where the degree of central pain experience significantly exceeds what the peripheral tissue would predict. Acknowledging this is not telling the patient the pain is in their head. It is telling them that their pain is real, that it has a neurological mechanism that current imaging does not capture, and that the treatment plan needs to address that mechanism as well as the peripheral driver.
Helping Patients Regain Control
The most powerful tool I have for helping patients who feel they have lost control of their pain is not a procedure or a prescription. It is clarity. Control comes from understanding the condition, seeing objective data, and having a step-by-step plan rather than a series of trials by error.
When I show a patient their nasal endoscopy in real time — when they can see the mucosal inflammation, the blocked drainage pathway, the biofilm-laden secretions that explain why antibiotics have not helped — something shifts. The pain that was invisible and inexplicable becomes visible and explicable. The patient who felt unseen becomes a patient with a map. That shift from confusion to clarity is often the most therapeutically significant moment in the entire clinical encounter, and it costs nothing except the time to explain it properly.
The patients I have seen make the most meaningful progress with chronic ENT pain are the patients who understood their condition thoroughly, who saw their own imaging, and who were given a sequential plan — not a single intervention with nothing behind it if it failed. Sequential planning — saline irrigation first, then allergy management, then topical therapy, then culture-directed treatment, then structural intervention if indicated — gives patients something to do at each stage. It removes the helplessness that chronic unresolved pain produces and replaces it with agency and momentum.
Dr. G’s Clinical Pearls
-
Pain in the head and neck is frequently referred. Where a patient feels pain is not necessarily where it originates. Face, ear, and throat symptoms routinely originate in other anatomical locations — and treating the location rather than the source produces consistently poor results.
-
Pain does not equal infection. The most common clinical error in primary care sinus management is reflexive antibiotic prescribing for pain that is inflammatory, pressure-driven, or neurological in origin. The 2025 AAO-HNS guideline confirms what rhinologists have observed for decades: most acute rhinosinusitis is viral and self-limiting, and most chronic rhinosinusitis is inflammatory rather than infectious.
-
The three-bucket framework — Structure, Inflammation, Nerve — is not a checklist. It is a clinical orientation that prevents premature anchoring on the most obvious explanation and keeps the differential open long enough to find the real driver.
-
Acute pain and chronic pain are different physiological phenomena requiring different treatment philosophies. Chronic ENT pain often reflects central sensitization — a rewired nervous system — not simply prolonged acute disease. Resetting a rewired system takes time and requires a plan that addresses nerve, tissue, and inflammatory pathways simultaneously.
-
The physical-psychological distinction in pain is clinically unhelpful. The airway is directly connected to the autonomic nervous system and the stress response. Emotional stress amplifies physical symptoms. Chronic physical inflammation impairs mood and cognition. Treating them as separate systems misses the mechanism that is sustaining both.
-
When patients can see their own imaging, watch their own endoscopy, and understand the clinical map of their condition — fear decreases, compliance increases, and outcomes improve. Clarity is therapeutic. Never underestimate the healing power of a visible plan.
-
The patients I have seen make the most meaningful progress with chronic ENT pain are patients who had three things: a clear diagnosis, objective data they could see with their own eyes, and a sequential treatment plan with a defined next step at every stage. Control comes from clarity and direction — not from procedures alone.
References
-
Rosenfeld RM, Piccirillo JF, Chandrasekhar SS, et al. Clinical Practice Guideline (Update): Adult Sinusitis. Otolaryngol Head Neck Surg. 2025;173(S1):S1-S56.
-
Prince AA, Steiger JD, Khalid AN, et al. Prevalence of biofilm-forming bacteria in chronic rhinosinusitis. Am J Rhinol. 2008;22(3):239-245.
-
Gould J, Alexander I, Tomkin E, Brodner D. In-office, multisinus balloon dilation: 1-year outcomes from a prospective, multicenter, open-label trial. Am J Rhinol Allergy. 2014;28(2):156-163.
-
Woolf CJ. Central sensitization: implications for the diagnosis and treatment of pain. Pain. 2011;152(3 Suppl):S2-S15.
-
Lumley MA, Cohen JL, Borszcz GS, et al. Pain and emotion: a biopsychosocial review of recent research. J Clin Psychol. 2011;67(9):942-968.
-
Bair MJ, Robinson RL, Katon W, Kroenke K. Depression and pain comorbidity: a literature review. Arch Intern Med. 2003;163(20):2433-2445.
-
Gergits FR. The Sinus Is the Victim, Pepsin Is the Perpetrator: Posterior Sinonasal Syndrome as the Etiological Precursor to Chronic Rhinosinusitis. Preprints. 2026. doi:10.20944/preprints202603.0858.v1
Want to Understand More?
This post is part of the Journal of Airway Inflammation on the Airway & Sinus Wellness Review.
→ Breaking the Biofilm: The Holistic Sinus Rinse Protocol for Recurring Sinus Infections
→ Why Antibiotics Keep Failing Your Sinus Infection
→ Does Balloon Sinuplasty Actually Work?
Airway & Sinus Wellness Review — Full Publication
Journal of Airway Inflammation — Clinical education from the Sinus & Allergy Wellness Center of North Scottsdale.
About the Author
Franklyn R. Gergits, DO, MBA, FAOCO is an otolaryngologist and rhinologist with over 30 years of clinical experience. He is the founder of the Sinus & Allergy Wellness Center of North Scottsdale, where he performs in-office balloon sinuplasty, turbinate reduction, NEUROMARK®, and swell body reduction procedures under local anesthesia. He performed the first balloon sinuplasty in Pennsylvania, holds dual Entellus Centers of Excellence certifications, and is the originator of the Posterior Sinonasal Syndrome (PSS) hypothesis, with a preprint available at Preprints.org (DOI: 10.20944/preprints202603.0858.v1). ORCID: 0009-0000-4893-6332.
SinusAndAllergyWellnessCenter.com · 480-525-8999
This content is for educational purposes only and does not constitute medical advice. If you are experiencing pain or sinus symptoms, please consult a qualified physician for evaluation and individualized treatment recommendations.
Disclaimer:
The information provided in this article is for informational and educational purposes only and does not constitute medical advice. It is not intended to diagnose, treat, cure, or prevent any disease or medical condition. Always seek the guidance of your physician or other qualified healthcare provider with any questions you may have regarding a medical condition or treatment.
Results may vary: Treatment outcomes and health experiences may differ based on individual medical history, condition severity, and response to care.
Emergency Notice: If you are experiencing a medical emergency, call 911 or seek immediate medical attention.
