Fifty Years of Rhinology — The Complete Story
Why Sinus Treatments Fail — And What Starts Before Them · Series Overview
The evolution of rhinology has given surgeons the best tools in history to treat sinus disease safely and effectively. The story of how we got those tools — and what we still do not fully understand — is the subject of an eight-chapter series on this publication. This article tells the complete arc of that story in a single read. For those who want to go deeper, each chapter is linked at the relevant point in the narrative.
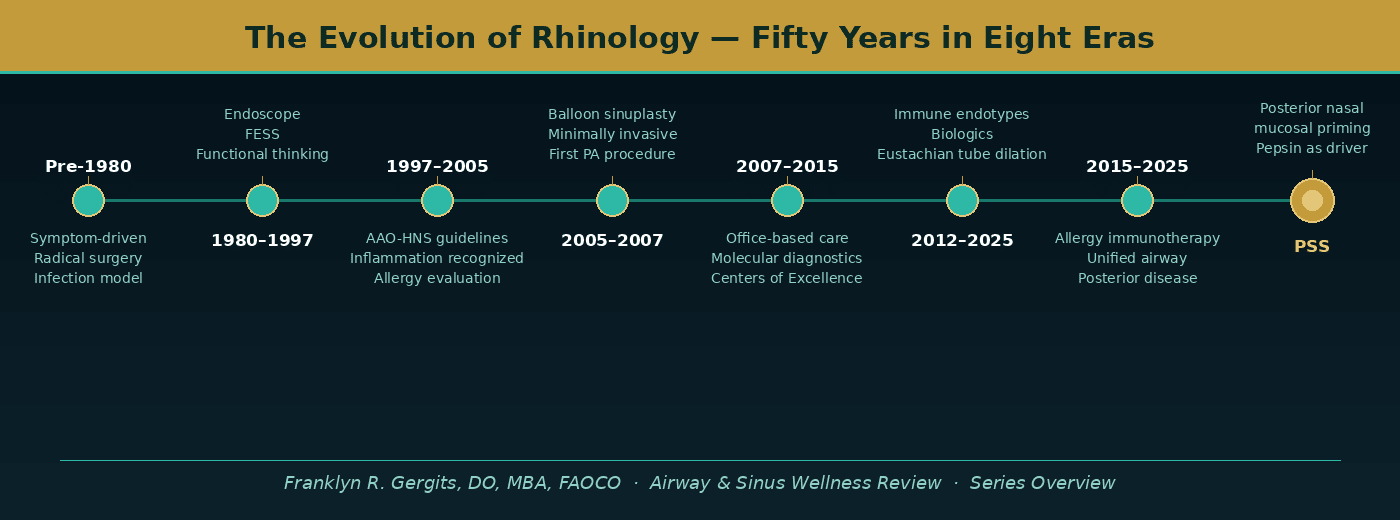
The graphic below shows the complete arc of rhinology’s evolution across eight distinct eras — from the symptom-driven, radical surgical approach of the pre-endoscopic era to the immune endotype revolution of the present day, and the clinical question that defines the field’s next chapter.
Each era built on what came before it, solved part of the problem, and revealed the next one. That progression — not any single breakthrough — is what made modern sinus care possible.
The Moment It All Clicked
Early February. Vail, Colorado. The Vanderbilt ENT Course — What’s New in ENT? Dr. James Duncavage, the lead rhinologist at Vanderbilt, was at the podium introducing a procedure that had never been performed in mainstream clinical practice before.
Balloon sinuplasty.
The idea was straightforward: guide a small flexible catheter into a blocked sinus opening, inflate a balloon to widen the drainage pathway, and restore normal function without cutting or removing tissue. The same principle that had transformed cardiovascular surgery when cardiac angioplasty replaced open-heart procedures for a generation of patients who might otherwise have waited too long.
That is the moment I understood what was happening. I could envision the impact immediately — the same way a cardiovascular surgeon must have felt the first time they heard about angioplasty. No more splitting sternums for every blocked coronary artery. No more patients waiting their turn for open-heart surgery only to succumb to a myocardial infarction (heart attack) while they waited. A new option. A less invasive protocol. A different pathway for the patients whose disease did not require the most aggressive intervention available.
All of those same situations apply to chronic rhinosinusitis (CRS). That realization — in a conference room in Colorado in early February — was my ah-hah moment. Dr. Reuben Setliff’s theory of “Small Hole Surgery” for the sinuses. It was all coming together. Everything that came before it, and everything that has come after it, makes more sense viewed from that single point of clarity.
Here is the fifty-year story that led there — and the question that is still being answered.
Before We Could See the Disease — Pre-1980
Before the endoscope, before the CT scan, before anyone had a framework for what was actually happening inside a blocked sinus, the field operated on a simple premise: sinus symptoms meant sinus infection, and infection required aggressive treatment.
Surgeons worked largely blind. Diagnosis depended on patient symptoms and plain radiographs that showed shadows rather than mucosal detail. The dominant surgical approach — the Caldwell-Luc procedure and intranasal ethmoidectomy — was designed to eradicate disease by removing as much tissue as possible. It worked for some patients. For others it created the next problem: scarring, mucosal loss, and a cascade of complications that would not be fully understood until a generation later.
The infection model made sense given what was knowable at the time. The surgery made sense given what was visible. The lesson that came out of this era was not that the surgeons were careless. They were not. The lesson was that you cannot fix what you cannot see — and the field was operating without the tools to see what it was actually treating.
→ Chapter 2: Before We Could See the Disease covers this era in full.
The Endoscopic Revolution — 1980 to 1997
The rigid nasal endoscope changed everything. When Walter Messerklinger in Austria began systematically examining the living nasal cavity through an endoscope, he saw something that no surgical textbook had adequately described: the disease was not where surgeons had been operating. The primary site of obstruction in most patients was not in the large sinuses — it was in the narrow drainage corridors of the anterior ethmoid and osteomeatal complex (OMC), where subtle mucosal swelling could block the drainage of multiple sinuses simultaneously.
Heinz Stammberger developed the surgical technique that followed from this observation. David Kennedy brought it to the United States and established Functional Endoscopic Sinus Surgery (FESS) as the new standard of care. The word functional was the key — the goal was no longer to remove disease by stripping tissue but to restore function by opening drainage pathways while preserving the mucosal lining that made the sinuses work.
The 1996 AAO-HNS (American Academy of Otolaryngology — Head and Neck Surgery) task force formalized this thinking into the first evidence-based guidelines for sinusitis management. For the first time the field had a shared framework — diagnostic criteria, treatment algorithms, and an agreed understanding of what chronic rhinosinusitis actually was.
FESS transformed outcomes for the majority of sinus patients. And it exposed the next question: why did a meaningful subset of patients still not get better, even after technically successful surgery?
→ Chapters 3 and 4 cover the endoscopic revolution and the first guidelines era.
Inflammation Enters the Conversation — 1997 to 2007
As the FESS era matured, it became increasingly clear that anatomy was not the whole story. Patients whose sinus openings were demonstrably patent — open, ventilated, functioning — continued to have recurrent symptoms. The field began to recognize what clinicians had been observing at the bedside for years: chronic rhinosinusitis was not primarily an infectious disease. It was primarily an inflammatory disease in which infection was often a secondary event.
Allergy evaluation became a standard component of CRS workup. The unified airway model — the recognition that the nose, sinuses, Eustachian (auditory) tubes, and lower airways share a common inflammatory biology — began to inform clinical practice. The 2003 and subsequent AAO-HNS guideline updates reflected this shift, incorporating allergy, immune evaluation, and medical management more formally into the treatment algorithm.
This era also produced the first serious discussion of disease heterogeneity — the recognition that not all CRS patients were the same and that the same treatment did not work for all of them. The field was beginning to ask why.
→ Chapter 5: The Guideline Era Redefined Disease covers this transition.
The Precision Era — 2007 to 2015
Two developments defined this era: the maturation of office-based procedural care and the introduction of molecular diagnostic technology.
Balloon sinuplasty — the procedure I first encountered at that Vanderbilt course in Vail — moved from hospital operating rooms to office procedure suites under local anesthesia. Reimbursement structures shifted to support office-based care. A subset of high-performing practices received formal designation as Sinus Centers of Excellence. I was among the first physicians to perform balloon sinuplasty in Pennsylvania, and I was designated a Sinus Center of Excellence — reflecting both clinical proficiency and a commitment to the office-based model that I believed was the right direction for appropriate CRS patients.
Molecular diagnostic technology — platforms like MicroGenDX using Next-Generation Sequencing (NGS) — entered rhinology practice and fundamentally changed how we understood what was living in the sinuses of patients who were not getting better. Standard culture missed the dominant organism in 53% of cases. DNA-based analysis identified polymicrobial infections, anaerobic organisms, fungal elements, and antimicrobial resistance genes that standard culture protocols could not detect. For the first time, treatment could be precisely directed at what was actually present rather than what the physician guessed might be present.
At SAWC, this technology became part of our intraoperative protocol — sampling directly from the sinus cavity at the time of balloon sinuplasty, delivering culture-directed topical antibiotic therapy into the newly opened spaces immediately after drainage was restored. Precision replaced empiricism. Local therapy replaced systemic overexposure.
→ Chapter 6: The Precision Era covers office-based rhinology and molecular diagnostics in full.
The Immune Era — 2012 to Present
The most intellectually significant development in modern rhinology was the recognition that chronic rhinosinusitis is not one disease. It is a heterogeneous collection of inflammatory processes — classified by immune endotype rather than by symptoms — that require fundamentally different treatment approaches depending on the underlying biology.
Type 2 inflammation — driven by specific cytokines including Interleukin-4 (IL-4), Interleukin-5 (IL-5), and Interleukin-13 (IL-13) — characterized patients with nasal polyps, tissue eosinophilia, and frequent comorbid asthma. This patient population responded to steroids and, ultimately, to biologic therapy. Dupilumab — a monoclonal antibody originally developed for eczema — produced dramatic improvements in polyp burden, smell, and quality of life in patients who had failed multiple surgeries and repeated medical courses. For the first time, the historic non-responder had a therapy that addressed the root biological driver of their disease.
Eustachian tube balloon dilation extended the reach of catheter-based technology to the ear. I attended the Harvard Endoscopic Surgery of the Sinuses, Eustachian Tube, and Ear Course in 2015, 2016, and 2017 — during the period when Dr. Dennis Poe was conducting the FDA clinical trials for the procedure. What resonated most from his teaching was the same principle that had guided my thinking since Vail: treat the upstream drivers. The Eustachian tube does not exist in isolation. Allergy, posterior sinonasal inflammation, and reflux all impair its function — and treating those drivers is inseparable from achieving durable outcomes.
Allergy immunotherapy — both subcutaneous (SCIT) and sublingual (SLIT) — became recognized not as an adjunct but as a foundational upstream driver treatment for a significant subset of CRS patients whose disease was maintained by ongoing allergic sensitization.
→ Chapter 7: The Immune Era covers biologics, Eustachian tube dilation, and allergy immunotherapy in full.
The Question the Field Still Needs to Answer
Fifty years of advancing technology have produced extraordinary tools. The endoscope. CT imaging. Functional surgical philosophy. Office-based procedures. Molecular diagnostics. Immune endotyping. Biologic therapy. Each generation of rhinologists has been given better tools than the last and has used them to help more patients than the generation before.
And yet a meaningful subset of patients — some with normal CT scans, some with successful surgical histories, some who do not fit the Type 2 endotype, some who have exhausted every available treatment — remain symptomatic. Their disease is real. Their frustration is legitimate. And the existing framework, as comprehensive as it has become, does not fully explain them.
The pattern I have observed in these patients across decades of clinical practice has a specific character. Symptoms that began posteriorly — throat clearing, globus sensation, ear fullness, chronic cough — long before the first sinus CT showed anything abnormal. Posterior nasal mucosal changes on endoscopy that do not fit established disease categories. A connection to meals, sleep position, and reflux physiology that suggests an upstream driver the field has not yet formally named.
The question I am proposing is this: could the posterior nasal cavity — primed by silent pepsin deposition from laryngopharyngeal reflux, inflamed through a mechanism that precedes and drives anterior sinus involvement — be the missing upstream driver that explains the patients the rest of the framework cannot?
That question is the foundation of the Posterior Sinonasal Syndrome (PSS) framework — a clinical hypothesis developed from thirty years of observing patients who did not fit the model, and from asking why the model left them behind. It is not the final chapter of rhinology’s evolution. It is the next question in a field that has always advanced by asking the right ones.
The full hypothesis is available as a preprint at Preprints.org: DOI https://doi.org/10.20944/preprints202603.0858.v1.
→ The Final Chapter: What the Field Still Cannot See presents the PSS framework in full.
Where to Start
If you are new to this series, the chapters are designed to be read in sequence — each one builds on the last. But if you want to jump directly to the era or topic most relevant to you, every chapter stands on its own.
For patients who have been told their sinuses are fine but still feel terrible — start with The Silent Years Before Your Sinus Diagnosis and the Final Chapter.
For clinicians and colleagues who want the complete clinical and historical argument — read the series from Chapter 2 through the Final Chapter in sequence.
For everyone: the history of rhinology is the history of open minds. Every advance came from someone who looked at a patient who was not getting better and asked a different question. That is still the work.
Franklyn R. Gergits, DO, MBA, FAOCO
Otolaryngologist & Rhinologist | 30+ Years Clinical Experience
Founder, Sinus & Allergy Wellness Center of North Scottsdale
SinusAndAllergyWellnessCenter.com · 480-525-8999
ORCID: 0009-0000-4893-6332
Preprint: https://doi.org/10.20944/preprints202603.0858.v1
This content is for educational purposes only and does not constitute medical advice.
Disclaimer:
The information provided in this article is for informational and educational purposes only and does not constitute medical advice. It is not intended to diagnose, treat, cure, or prevent any disease or medical condition. Always seek the guidance of your physician or other qualified healthcare provider with any questions you may have regarding a medical condition or treatment.
Results may vary: Treatment outcomes and health experiences may differ based on individual medical history, condition severity, and response to care.
Emergency Notice: If you are experiencing a medical emergency, call 911 or seek immediate medical attention.
