The Final Chapter: What the Field Still Cannot See
Why Sinus Treatments Fail — And What Starts Before Them · The Final Chapter of the Series
Keywords: Posterior Sinonasal Syndrome (PSS), Laryngopharyngeal Reflux (LPR), Pepsin, Posterior Nasal Nerve, Neuromark, Chronic Rhinosinusitis (CRS), Airway Inflammation, Systemic Inflammation, Mucosal Priming, Antibiotic Stewardship, Unified Airway, Field Cancerization, Mucosal-Preserving Surgery, Rhinology Evolution, AAO-HNS Guidelines.
The Question That Started This
Every clinician who treats sinus and airway disease has heard a version of this:
“Can you please just give me an antibiotic already?”
The patient sitting across from you is not being difficult. They are exhausted. They have heard the explanations. They understand — intellectually — that antibiotics are not the answer for most sinus episodes. But they are in pain, they cannot breathe, they have a meeting tomorrow, and they do not have time for the full anti-inflammatory protocol you are recommending. They want relief. They want it now. And they want to know — specifically, precisely, honestly — what treatment pathway will actually make them feel better as soon as possible.
That question is not unreasonable. It is, in fact, the most important clinical question in all of rhinology — because the honest answer exposes everything the field has not yet fully solved.
This series has traced the evolution of that honest answer across fifty years of rhinology. What began as symptom-based diagnosis and radical surgery became endoscopy and functional thinking, then guidelines and inflammation, then precision diagnostics and office-based care, then immune endotypes and biologic therapy. Each era answered part of the question. None of them answered all of it.
This final chapter is about the part that is still unanswered — and about a clinical framework that may be the missing piece.
The Moment the Question Changed
I have been treating sinus and airway disease for over thirty years. In that time I have performed thousands of procedures, managed countless courses of medical therapy, and watched the field develop tools that would have seemed extraordinary to the physicians who trained me.
And yet the patients who have stayed with me most persistently are not the ones who got better. They are the ones who did not — despite everything the field had to offer.
The moment my thinking shifted happened when I began to learn about the treatment of posterior nasal nerve overactivity — specifically the Neuromark procedure, which uses targeted radiofrequency energy to modulate the posterior nasal nerve and reduce the parasympathetic hypersecretion driving chronic posterior nasal symptoms.
What I noticed — and what I could not stop thinking about — was this: patients who underwent posterior nasal nerve treatment were reporting improvement in symptoms that had nothing obviously to do with nerve function. Their sinus pressure improved. Their postnasal drainage decreased. Their sleep quality got better. Their recurrent infections became less frequent.
I could understand the anterior osteomeatal complex (OMC) focus. Opening the anterior drainage pathways has real impact for most patients — that is established, documented, and reproducible. But the posterior nerve treatment was reducing symptoms in patients whose anterior disease had already been addressed. Patients who had had technically successful surgery. Patients who were coming to me for second opinions after cycling through treatment after treatment without resolution.
The posterior nasal cavity was doing something that the anterior-focused model of sinus disease could not explain.
That observation was the beginning of what eventually became the Posterior Sinonasal Syndrome (PSS) framework.
The Hidden Driver — Pepsin and the LPR Connection
Running parallel to my clinical observations about posterior nasal nerve overactivity was a growing body of evidence about a molecule that most rhinologists had never considered as a driver of chronic sinonasal disease.
Pepsin — a proteolytic enzyme produced in the stomach for the digestion of proteins — has been detected in the mucosa of the nasopharynx, the middle ear, the larynx, and the sinonasal cavity in patients with Laryngopharyngeal Reflux (LPR). Unlike gastric acid, which is rapidly buffered and neutralized once it exits the esophagus, pepsin is remarkably stable at physiologic pH levels and can be reactivated by even mildly acidic conditions — including the pH fluctuations that occur in the posterior nasal cavity during normal breathing.
What pepsin does to the posterior nasal mucosa is not a simple irritation. Through a process of receptor-mediated endocytosis — the cell actively taking up pepsin from the mucosal surface — pepsin enters the epithelial cells lining the posterior nasal cavity and drives an inflammatory cascade from within. It depletes protective surface proteins. It activates pro-inflammatory signaling pathways including Nuclear Factor kappa B (NF-κB). It increases mucin production. It impairs mucociliary clearance. And it does all of this silently — without producing the acid taste, the heartburn, or the classic reflux symptoms that would prompt a patient or physician to consider gastroesophageal or laryngopharyngeal reflux as part of the clinical picture.
This is the hidden driver. Not the antibiotic-resistant bacteria — though those are real. Not the allergy that was inadequately treated — though that matters too. Not the anatomy that was not quite opened enough — though surgical technique is always relevant. The hidden driver, in a meaningful proportion of patients with recurrent and treatment-refractory chronic rhinosinusitis, is a digestive enzyme reaching the posterior nasal mucosa during episodes of silent reflux — most often at night, while the patient lies flat, while the protective mechanisms of the upright waking state are suspended.
The therapeutic implication of this recognition has been universally accepted as clinically relevant in the laryngopharyngeal reflux literature for over a decade. What has not yet been fully accepted — and what this series is built to argue — is that the same pepsin-driven inflammatory pathway operates upstream of the sinuses themselves, priming the posterior nasal mucosa for recurrent disease long before the first CT scan shows anything abnormal.
Posterior Sinonasal Syndrome — The Framework
Posterior Sinonasal Syndrome (PSS) is a clinical framework built on a single organizing observation: in a significant subset of patients with recurrent acute rhinosinusitis, chronic rhinosinusitis, and treatment-refractory sinus disease, the primary driver of disease is not located in the sinuses. It is located in the posterior nasal cavity — in the mucosa of the nasopharynx and posterior nasal septum — where silent pepsin deposition from laryngopharyngeal reflux creates a state of chronic mucosal priming that lowers the threshold for sinus involvement, perpetuates neurogenic inflammation through posterior nasal nerve activation, and generates symptoms that are indistinguishable from classic sinusitis but do not respond to treatments directed at the sinuses themselves.
The PSS model explains several clinical observations that the existing rhinology framework cannot adequately account for:
Why some patients with minimal CT findings have severe and persistent symptoms. Why some patients with technically successful sinus surgery continue to have recurrent episodes at the same frequency as before the procedure. Why posterior nasal nerve treatment reduces sinus symptoms in patients whose sinus anatomy has already been optimized. Why alkaline water, alginate barrier therapy, and dietary acid elimination produce symptom improvement in patients with no classic reflux complaints. Why the symptom burden in some patients fluctuates with meals, sleep position, alcohol consumption, and stress in ways that correlate with reflux physiology rather than infection patterns.
PSS does not replace the existing diagnostic framework. Anatomical obstruction is real. Allergic inflammation is real. Immune deficiency is real. Biofilm-forming bacteria are real. Each of those drivers requires its own identification and treatment. What PSS adds is a recognition that posterior mucosal inflammation from pepsin deposition can operate simultaneously with all of those drivers — or independently of them — and that failing to identify and treat it leaves a significant proportion of patients without a complete explanation for their disease.
The Five-Stage Clinical Progression
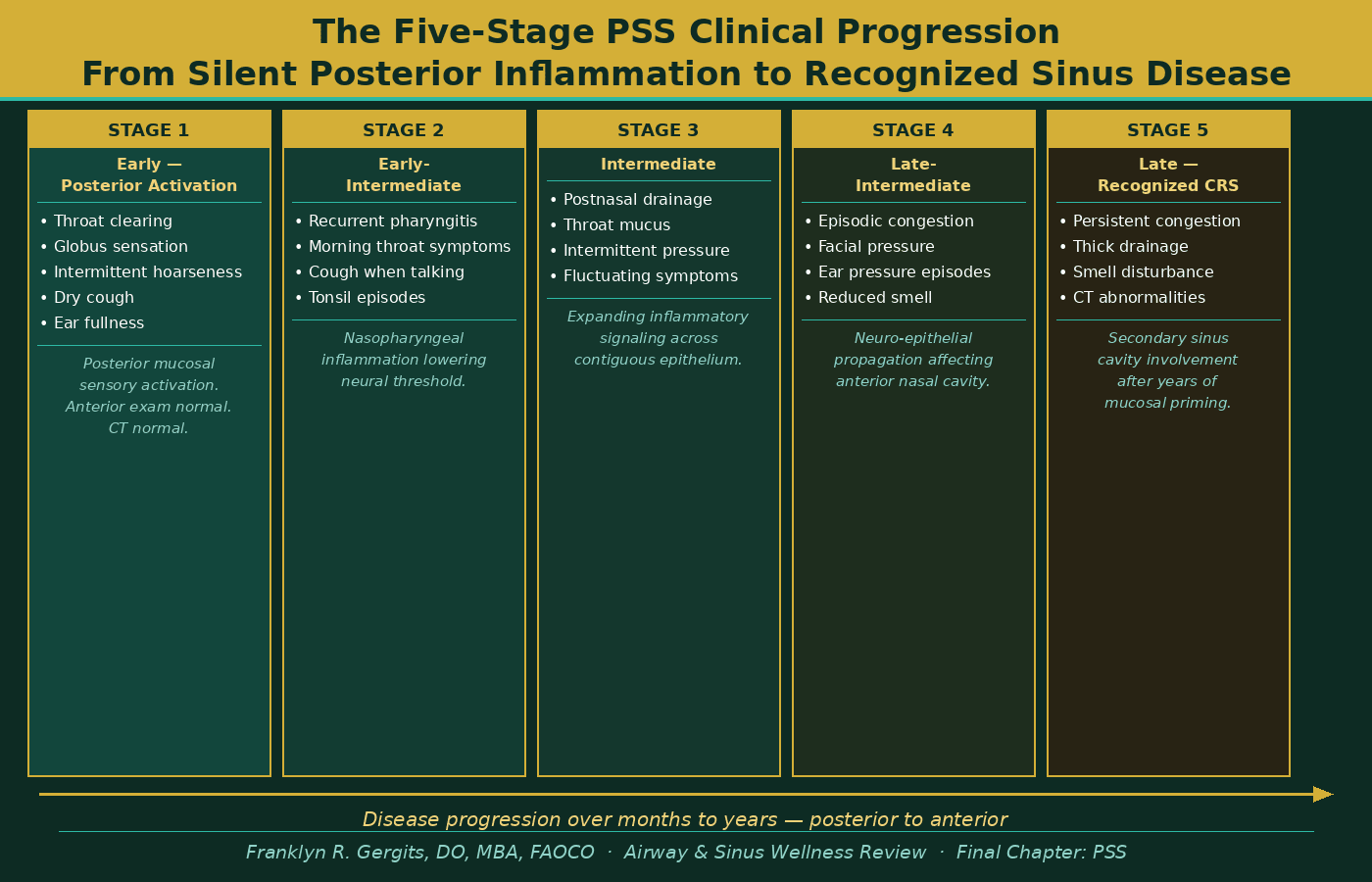
In clinical practice, PSS presents as a predictable progression of symptoms that begins posteriorly and moves anteriorly over time — often over years or even decades before the first sinus diagnosis is made.
The earliest stage is characterized by posterior activation — throat clearing that never fully resolves, a globus sensation, intermittent hoarseness without laryngeal pathology, a dry cough that appears when talking or laughing, and ear fullness that audiometry cannot explain. At this stage the anterior nasal exam is normal. The CT scan is normal. The patient is told they may have reflux, or allergies, or anxiety, or a post-viral cough. They are not told they may have the early stages of a posterior inflammatory process that will, over time, prime their sinuses for the recurrent disease that lies ahead.
As posterior mucosal inflammation becomes established and the neural activation threshold in the nasopharynx drops, the intermediate stages follow — recurrent pharyngitis, postnasal drainage that thickens and persists between apparent infections, episodic sinus pressure without objective obstruction, and Eustachian tube dysfunction driven not by anatomical blockage but by nasopharyngeal inflammation directly adjacent to the Eustachian tube orifice.
The late stage — recognized chronic rhinosinusitis with CT abnormalities and documented mucosal disease — is where most patients first enter the rhinology system. But by this point the posterior inflammatory process has been active for years. The sinus involvement is real. But it is secondary. It is the downstream consequence of a posterior driver that is still operating and will continue to operate regardless of what is done to the sinuses themselves.
This is why the sinus is the victim. And pepsin is the perpetrator.
Figure 1 illustrates the five-stage progression of Posterior Sinonasal Syndrome — from the earliest posterior mucosal activation, which is frequently missed or misdiagnosed, through the intermediate stages of expanding neurogenic inflammation, to the late-stage recognized chronic rhinosinusitis that finally brings the patient into the rhinology system. The critical insight this progression reveals is that by the time the sinuses are visibly involved, the posterior inflammatory process has been active for months or years.
What the Anti-Pepsin Treatment Pathway Looks Like
For the patient sitting across from you asking for the antibiotic — the one who does not have time for the full protocol — the honest answer to their question requires understanding which driver is actually operating in their case. If their disease is anatomically driven, surgery is the answer. If it is allergically driven, immunotherapy is the answer. If it is immune-mediated Type 2 disease, biologics may be the answer. And if it is pepsin-driven posterior mucosal inflammation — PSS — the treatment pathway looks nothing like any of those.
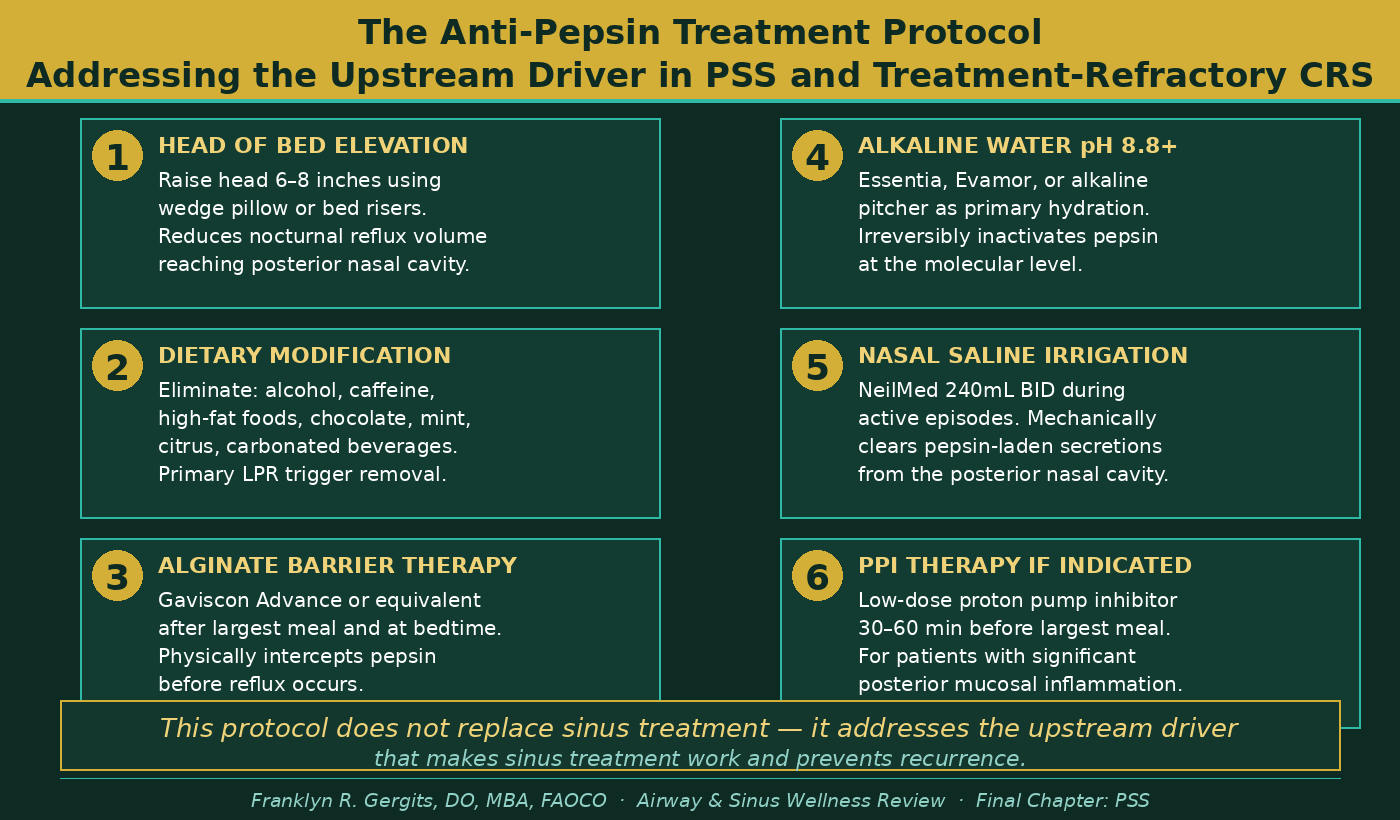
The anti-pepsin protocol is not complicated. It is not expensive. It does not require a prescription in most cases. But it requires consistency, because pepsin deposition is a nightly event in susceptible patients and the mucosal damage accumulates gradually.
The foundational elements are: head of bed elevation to reduce nocturnal reflux volume; dietary elimination of the primary reflux triggers — alcohol, caffeine, high-fat meals, acidic foods, chocolate, mint; alginate barrier therapy after the largest meal of the day and at bedtime, physically intercepting pepsin before it can reach the esophageal and pharyngeal mucosa; alkaline water at pH 8.8 or above as the primary hydration source, which irreversibly inactivates pepsin at the molecular level; and nasal saline irrigation that mechanically clears pepsin-laden secretions from the posterior nasal cavity before they can be reactivated by local pH changes.
For patients with significant posterior mucosal inflammation on endoscopy — the cobblestoning, the lymphoid hyperplasia, the thick posterior secretions that do not respond to antibiotic therapy — the addition of low-dose proton pump inhibitor (PPI) therapy directed specifically at reducing the acid activation of pepsin during reflux episodes provides an additional layer of protection that mechanical and dietary measures alone cannot achieve.
This is not a replacement for treating the sinuses. It is what makes treating the sinuses work.
Figure 2 outlines the six-step anti-pepsin protocol used at the Sinus and Allergy Wellness Center of North Scottsdale for patients with confirmed or suspected Posterior Sinonasal Syndrome. This protocol addresses the upstream pepsin-driven inflammatory driver directly — not as a replacement for sinus treatment, but as the foundation that makes sinus treatment work and prevents the recurrence that has frustrated both patients and clinicians for decades.
An Open Letter to Every Clinician Who Has Run Out of Answers
If you have read this entire series — from the radical surgery of the pre-endoscopic era through the precision diagnostics of the 2010s to the biologic revolution of the present day — and you recognize in these pages the patients who have frustrated you most, then this final section is written directly for you.
Keep an open mind.
The history of rhinology is the history of open minds. Messerklinger kept an open mind when he looked through an endoscope and saw that the disease was not where surgeons had been operating. Kennedy kept an open mind when he brought that technology to a skeptical American rhinology community. The investigators who designed the first biologic trials kept an open mind when they asked whether a medication developed for eczema might change the biology of nasal polyps.
Every advance in this field — without exception — required someone to look at a patient who was not getting better and ask a different question than the one the existing framework suggested.
The AAO-HNS guidelines that have provided our specialty — and every specialty that touches airway disease — with best practices have evolved continuously because the physicians who contributed to them kept an open mind as new evidence emerged. Those guidelines will continue to evolve. The current understanding of CRS endotypes, biologic therapy, and posterior disease recognition is not the final word. It is the best current word, which is a different thing entirely.
Our knowledge changes as our understanding improves. That is not a weakness of the field. It is the definition of a field that is working correctly.
What I am asking you to consider — as a colleague, as a fellow clinician who has sat across from the same exhausted, frustrated, not-getting-better patients — is whether the posterior nasal cavity deserves the same systematic attention that the anterior osteomeatal complex has received for the past four decades. Whether the pepsin molecule deserves the same clinical suspicion in refractory rhinosinusitis that resistant bacteria and immune deficiency have earned. Whether a patient whose symptoms began with throat clearing and ear fullness years before their first sinus CT deserves a framework that explains that trajectory rather than treating each episode as if it occurred in isolation.
I believe it does. I believe they deserve that framework. And I believe the field is ready to build it — because the tools already exist, the evidence is accumulating, and the patients who need it have been waiting long enough.
Where This Goes Next
The Posterior Sinonasal Syndrome hypothesis is available in full as a preprint at Preprints.org — indexed, citable, and permanently timestamped at DOI: https://doi.org/10.20944/preprints202603.0858.v1.
The research agenda that follows from this framework includes prospective validation of the nasal lavage pepsin assay as an objective diagnostic biomarker for PSS, clinical outcomes studies of anti-pepsin treatment in PSS-confirmed patients, investigation of the relationship between posterior nasal pepsin burden and sinonasal field cancerization risk, and characterization of the five-stage PSS progression in a prospective patient cohort.
None of that research can happen without clinical awareness. And clinical awareness begins with the kind of series you have just read — the honest, complete account of how we got here, what we built, what we solved, and what we have not yet solved.
The sinus is the victim. Pepsin is the perpetrator. And the field that has spent fifty years perfecting its tools for the victim is ready — I believe — to turn its attention to the perpetrator.
Dr. G’s Clinical Pearls — The Final Chapter
-
The question “can you please just give me an antibiotic” is not unreasonable — it is the most important clinical question in rhinology, because the honest answer exposes everything we have not yet solved
-
Posterior nasal nerve overactivity producing anterior sinus symptoms was the clinical observation that opened the PSS framework — the posterior nasal cavity is not a passive bystander in sinus disease
-
Pepsin is stable at physiologic pH, reactivatable by mild acidity, and capable of driving mucosal inflammation through receptor-mediated endocytosis — silently, without classic reflux symptoms
-
PSS does not replace the existing diagnostic framework — it adds the posterior inflammatory driver that the existing framework does not account for
-
The symptom progression in PSS begins posteriorly — throat clearing, globus, ear fullness — years before the first sinus CT shows anything abnormal
-
The anti-pepsin protocol is not complicated — head of bed elevation, dietary modification, alginate barrier therapy, alkaline water, and nasal saline irrigation form the foundation
-
Our knowledge changes as our understanding improves — that is not a weakness, it is the definition of a field working correctly
-
Every advance in rhinology required someone to look at a patient who was not getting better and ask a different question
-
The field is ready to ask that question about the posterior nasal cavity — the patients who need it have been waiting long enough
Reference List — Final Chapter
1. Johnston N et al. Pepsin as a causal agent of inflammation during nonacidic reflux. Otolaryngol Head Neck Surg. 2004;130:649–652.
2. Johnston N et al. Receptor-mediated uptake of pepsin by laryngeal epithelial cells. Ann Otol Rhinol Laryngol. 2007;116:934–938.
3. Koufman JA, Johnston N. Potential role of pepsin in the pathogenesis of laryngeal inflammation. Ann Otol Rhinol Laryngol. 2012;121(5):327–332.
4. Samuels TL, Johnston N. Pepsin as a marker of extraesophageal reflux. Ann Otol Rhinol Laryngol. 2010;119:203–208.
5. Koufman JA, Johnston N. Potential benefits of pH 8.8 alkaline drinking water as an adjunct in the treatment of reflux disease. Ann Otol Rhinol Laryngol. 2012;121:431–434.
6. Rees LE et al. The laryngeal epithelial barrier: a new consideration in reflux disease pathogenesis. Laryngoscope. 2008;118:966–971.
7. Strugala V et al. A randomized controlled trial to investigate the efficacy and safety of a novel alginate compound in a mixed reflux population. J Laryngol Otol. 2010;124:1023–1028.
8. McGlashan JA et al. The effect of an alginate-based compound on symptoms of laryngopharyngeal reflux. J Laryngol Otol. 2009;123:1020–1024.
9. Li S et al. Pepsin detection in nasopharyngeal carcinoma tissue. Cancer Biomark. 2019;25:375–381.
10. Crapko M et al. Role of extra-esophageal reflux in chronic otitis media with effusion. Laryngoscope. 2007;117:1419–1423.
11. Poelmans J, Tack J. Extraoesophageal manifestations of gastro-oesophageal reflux. Gut. 2005;54:1492–1499.
12. Numminen J et al. Chronic rhinosinusitis and Helicobacter pylori — is there a link? Eur Arch Otorhinolaryngol. 2011;268:1337–1340.
13. Fokkens WJ et al. European Position Paper on Rhinosinusitis and Nasal Polyps 2020 (EPOS 2020). Rhinology Suppl. 2020;29:1–464.
14. Rosenfeld RM et al. Clinical Practice Guideline (Update): Adult Sinusitis. Otolaryngol Head Neck Surg. 2015;152(2 Suppl):S1–S39.
15. Bachert C et al. Dupilumab efficacy and safety in patients with severe chronic rhinosinusitis with nasal polyps. Lancet. 2019;394:1638–1650.
16. Hens G, Hellings PW. The nose: gatekeeper and trigger of bronchial disease. Rhinology. 2006;44:179–187.
17. Hellings PW et al. Uncontrolled allergic rhinitis and chronic rhinosinusitis. Allergy. 2013;68:1–7.
18. Messerklinger W. Endoscopy of the Nose. Baltimore: Urban and Schwarzenberg; 1978.
19. Kennedy DW et al. Endoscopic sinus surgery — analysis of 100 patients. Laryngoscope. 1987;97:421–429.
20. Stammberger H. Functional Endoscopic Sinus Surgery. Philadelphia: BC Decker; 1991.
21. Gergits FR. The Sinus Is the Victim, Pepsin Is the Perpetrator: Posterior Sinonasal Syndrome as the Etiological Precursor to Chronic Rhinosinusitis, Field Carcinogen of the Upper Aerodigestive Tract, and the Biological Imperative for Mucosal-Preserving Surgery. Preprints 2026. DOI: 10.20944/preprints202603.0858.v1.
Franklyn R. Gergits, DO, MBA, FAOCO
Otolaryngologist & Rhinologist | 30+ Years Clinical Experience
Founder, Sinus & Allergy Wellness Center of North Scottsdale
SinusAndAllergyWellnessCenter.com · 480-525-8999
ORCID: 0009-0000-4893-6332
Preprint: https://doi.org/10.20944/preprints202603.0858.v1
This content is for educational purposes only and does not constitute medical advice. If you are experiencing severe symptoms, orbital swelling, high fever, or neurological changes, seek immediate medical care.
Disclaimer:
The information provided in this article is for informational and educational purposes only and does not constitute medical advice. It is not intended to diagnose, treat, cure, or prevent any disease or medical condition. Always seek the guidance of your physician or other qualified healthcare provider with any questions you may have regarding a medical condition or treatment.
Results may vary: Treatment outcomes and health experiences may differ based on individual medical history, condition severity, and response to care.
Emergency Notice: If you are experiencing a medical emergency, call 911 or seek immediate medical attention.
