The Glymphatic System: How Your Brain Cleans Itself While You Sleep
Most patients who come to me with chronic sinus disease are thinking about their nose. They are thinking about congestion, pressure, drainage, and the recurring infections that have defined their daily existence for months or years. They are not thinking about their brain.
They should be.
There is a system inside the brain — discovered only in 2013 — that cleans the brain of its own inflammatory waste products during sleep. It is called the glymphatic system. And in a patient with nasal obstruction, chronic sinus disease, and the fragmented sleep that inevitably follows, that system is not working the way it should. The consequence is not just poor sleep. It is an accumulating neuroinflammatory burden that the patient experiences as brain fog, cognitive difficulty, fatigue, and a persistent sense of not being fully present — symptoms they have been told have nothing to do with their sinuses.
They have everything to do with their sinuses.
Clinical science from the Journal of Airway Inflammation — published by the Airway & Sinus Wellness Review. Subscribe for weekly rhinology and airway inflammation research.
What the Glymphatic System Is — and Why It Took Until 2013 to Find It
The glymphatic system is, in the simplest terms, the brain’s version of the lymphatic system. Where the peripheral lymphatic system moves inflammatory fluid and debris through channels in the body’s tissues, the glymphatic system moves a specific fluid — cerebrospinal fluid — through channels alongside the brain’s blood vessels, flushing the brain’s own metabolic waste products out of the neural tissue and into the peripheral lymphatic system for clearance.
The reason it took until 2013 for science to document this system is straightforward: the brain has no obvious lymphatic channels and no lymph nodes of its own. For generations, neuroscientists operated on the assumption that the brain was immunologically privileged — that its waste clearance happened through mechanisms that did not involve the lymphatic system at all. When Dr. Maiken Nedergaard and her team at the University of Rochester demonstrated the glymphatic pathway in 2013, it required new imaging techniques — two-photon microscopy and tracer injection studies in living mice — that simply had not existed before. The channels are microscopic, they run alongside the brain’s smallest blood vessels, and they are managed by a specific type of brain cell — the astrocyte — whose role in CSF movement had not previously been understood.1
The name glymphatic is a combination of glial — referring to the astrocyte cells that manage the system — and lymphatic, acknowledging the functional similarity to the peripheral lymphatic network. The system works through a remarkably elegant mechanism. Cerebrospinal fluid flows inward along the spaces surrounding the brain’s arteries, driven by arterial pulsation. It mixes with the interstitial fluid — the fluid bathing the brain’s neurons — exchanging through channels in the astrocyte membrane controlled by a protein called aquaporin-4. The mixed fluid then exits along the spaces surrounding the brain’s veins, carrying with it the metabolic waste products — including amyloid beta and tau — that accumulate during the brain’s waking activity.1,2
That outflowing waste does not simply disappear. It drains into the meningeal lymphatic vessels — a network of lymphatic channels running along the brain’s outer covering — and from there into the cervical lymph nodes and ultimately into systemic circulation for elimination.3 The glymphatic system and the peripheral lymphatic system are not separate entities. They are two stages of a single continuous waste clearance pathway that begins in the brain and ends in the body’s lymphatic network.
What Happens During Deep Sleep — The Cleaning Cycle
The glymphatic system is not equally active at all times. Its function is dramatically and specifically linked to sleep — particularly to the deep, slow-wave stages of sleep that the brain enters during the first half of the night.
During waking hours, the brain is metabolically active. Neurons are firing, neurotransmitters are being synthesized and released, inflammatory byproducts are accumulating in the interstitial space between cells. The glymphatic system is operating during waking — but at a fraction of its sleep capacity. The brain during waking is a factory running at full production. Cleaning happens, but it cannot keep pace with the output.
During slow-wave sleep — the deep, restorative stages characterized by large, synchronized delta waves — something remarkable happens. The brain’s neurons actually contract slightly. The interstitial space between cells expands by as much as 60 percent compared to the waking state. This expansion dramatically increases the volume of cerebrospinal fluid that can flow through the perivascular channels, and the rate of glymphatic clearance increases by a factor of two or more compared to waking.1 The factory has shut down production, the floor has been cleared, and the cleaning crew has moved in with full access.
This is the cleaning cycle. It is not metaphorical. It is a measurable, documented biological event that happens in the brain every night — but only when slow-wave sleep is achieved, sustained, and repeated across multiple cycles. The fluid flows in, mixes with the interstitial waste, carries the debris out along the venous channels, and drains toward the cervical lymph nodes. Then the next cycle begins. By morning, a brain that has slept well has cleared the neuroinflammatory accumulation of the previous day and reset for another cycle of waking activity.
A brain that has not slept well has not done this. The debris remains. The amyloid beta and tau accumulate. The inflammatory load carries forward into the next day — and the next, and the next. The patient wakes up feeling as though they never fully recovered from the previous day. Because they did not.
Nasal Obstruction, Fragmented Sleep, and the Glymphatic Failure Cascade
Here is where the sinus patient’s story connects directly to the glymphatic system.
Nasal airway obstruction — from a deviated septum, from turbinate hypertrophy, from chronic mucosal inflammation, from the structural and inflammatory consequences of chronic sinus disease — changes the way a person breathes during sleep. The increased resistance to airflow forces the sleeping patient to work harder to move air through the narrowed passages. This increased effort alters sleep architecture in a specific and well-documented way: the proportion of time spent in light sleep increases, and the proportion of time spent in deep slow-wave sleep decreases.
The patient does not experience this as waking up. They experience it as never feeling fully rested regardless of how many hours they spend in bed. They describe sleeping eight hours and waking up exhausted. They describe an afternoon fatigue that arrives without fail every day at the same time. They describe a persistent cognitive fog that makes word retrieval slower, concentration harder, and decision-making more effortful than it used to be. They attribute these symptoms to stress, to getting older, to working too hard. They do not connect them to their nose.
But the connection is direct. Less slow-wave sleep means less glymphatic flow. Less glymphatic flow means less clearance of amyloid beta, tau, and the other neuroinflammatory byproducts of the day’s neural activity. That accumulating neuroinflammatory burden is experienced as brain fog, cognitive drift, and fatigue. When the nasal airway is restored — through in-office turbinate reduction, balloon sinuplasty, or in some cases septoplasty — sleep architecture improves. The proportion of slow-wave sleep increases. Glymphatic clearance improves. And patients come back to tell us something we hear consistently but that still surprises them every time: they did not realize how poorly they had been sleeping until they experienced the difference.
That improvement in cognitive clarity, in morning energy, in the sense of being mentally present — it is not a placebo effect. It is the glymphatic system being restored to function.
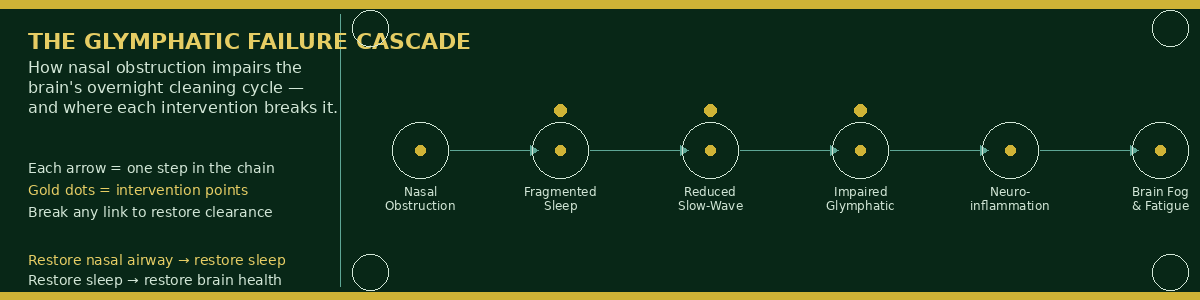
The diagram below maps the cascade from nasal obstruction through fragmented sleep to glymphatic failure and neuroinflammatory accumulation — showing exactly where each intervention in the protocol interrupts the cycle.
Amyloid, Tau, and the Alzheimer’s Connection
Among the waste products that the glymphatic system clears during sleep, two have received significant scientific attention: amyloid beta and tau protein. These are the same proteins that accumulate in the brains of patients with Alzheimer’s disease — amyloid beta forming the plaques and tau forming the tangles that characterize the disease pathologically.
The glymphatic system is the primary mechanism by which the brain clears amyloid beta from the interstitial space during sleep.4 When glymphatic function is impaired — whether by sleep deprivation, by chronic sleep fragmentation from nasal obstruction, or by the reduction in glymphatic capacity that occurs with normal aging — amyloid beta accumulates at a rate that exceeds the brain’s ability to clear it. Over time, the concentration increases. The risk of Alzheimer’s disease rises.
These two proteins must be cleared continuously. The slow, incremental increase in their concentration — driven by years of fragmented sleep and impaired glymphatic function — creates a progressively higher risk for the development of this devastating disease. This is not a theoretical concern for patients with a family history of Alzheimer’s. It is a documented biological mechanism with a directly addressable upstream driver.
For any patient who comes to me with chronic nasal obstruction and a family history of Alzheimer’s disease or early dementia — a parent, a grandparent, a sibling — I want them to understand this connection completely. Every possible avenue for reducing their risk needs to be pursued. Sleep quality and the maximization of glymphatic clearance is one of those avenues. Reducing the nasal obstruction that fragments their sleep is one of the most concrete, actionable steps available. Restoring the nasal airway in these patients is not just a quality of life intervention. In the context of everything we now know about glymphatic function and neurodegeneration risk, it may be a preventive one.
The PSS Connection — When Pepsin Reaches the Brain’s Drainage Pathway
There is a connection between the glymphatic system and the Posterior Sinonasal Syndrome (PSS) hypothesis that I believe has not yet been formally described in the literature — but that the science supports.
Clinical Hypothesis — Dr. Franklyn R. Gergits, DO, MBA, FAOCO
The Posterior Sinonasal Syndrome (PSS) proposes that pepsin — the proteolytic enzyme produced in the stomach — reaches the posterior nasal cavity via silent laryngopharyngeal reflux during sleep. Once deposited on the posterior sinonasal mucosa, pepsin is internalized by epithelial cells and activates inflammatory signaling cascades that drive chronic sinonasal mucosal disease.
The mucociliary clearance system — the same system that propels airway contents posteriorly toward the nasopharynx — is also the pathway through which anterior sinonasal inflammation, allergens, viruses, bacteria, and environmental irritants concentrate in the posterior nasal cavity. The anatomy of the posterior nasal cavity funnels and concentrates this inflammatory burden as the passages narrow. This is the anatomical basis of PSS.
The connection to the glymphatic system is this: the meningeal lymphatic vessels — through which the glymphatic system drains its output — exit the brain through the cribriform plate and through foramina at the skull base in proximity to the posterior nasal cavity and the nasopharynx. A chronic inflammatory environment in the posterior sinonasal space — whether driven by pepsin, by concentrated allergen and microbial burden, or by the structural consequences of long-standing CRS — creates an inflammatory milieu in direct anatomical proximity to these drainage pathways.
Whether posterior sinonasal inflammation impairs meningeal lymphatic function and thus downstream glymphatic clearance capacity is a testable hypothesis that has not yet been studied. I propose it here as a direction for future investigation — and as a clinical rationale for treating posterior sinonasal disease with the same urgency we bring to structural nasal obstruction in the context of glymphatic health and neurodegeneration risk.
Furthermore, pepsin is now linked to laryngeal cancer and nasopharyngeal cancer — the first two confirmed cancer associations with this enzyme’s extra-esophageal presence. I propose that as the research expands, pepsin’s role in the development of other head and neck cancers will be established. The implication is significant: posterior sinonasal disease is not merely a quality-of-life condition. In patients with sustained pepsin exposure in the posterior nasal cavity and nasopharynx, it may be a pre-malignant condition requiring the same clinical urgency we bring to other recognized cancer precursors.
Preprint DOI: 10.20944/preprints202603.0858.v1 · Manuscript under review, Laryngoscope Investigative Otolaryngology
The Glymphatic Optimization Protocol — Starting Tonight
The good news is that glymphatic function responds to behavioral interventions that are available to every patient immediately — without a prescription, without a procedure, and without waiting for a specialist appointment. The protocol below is what I recommend to every patient in my practice with brain fog, cognitive difficulty, morning fatigue, or a family history of Alzheimer’s disease.
The SAWC Glymphatic Optimization Protocol
Step 1: Sleep Hygiene — The Foundation
Glymphatic clearance is entirely dependent on achieving and sustaining slow-wave sleep. Everything else in this protocol supports that goal. Sleep hygiene is not optional self-care advice — it is the primary clinical intervention.
-
Consistent sleep and wake time — the single most powerful circadian regulator available without medication. The brain’s glymphatic system is tuned to a biological clock. Irregular schedules disrupt the timing of slow-wave sleep entry and reduce total clearance time.
-
Stop screen exposure 45–60 minutes before sleep — blue light suppresses melatonin secretion and delays sleep onset. This is not a suggestion. It is a physiological fact.
-
No vigorous exercise within 2–3 hours of sleep — exercise raises core body temperature and sympathetic nervous system activity, both of which delay slow-wave sleep entry
-
Dark, cool room — 65–68°F is the documented optimal range for sleep initiation and maintenance. Light exposure during sleep suppresses melatonin even through closed eyelids.
-
Bed is for sleep only — not for television, laptop work, or prolonged phone use. The association between the bed environment and wakefulness is a learned response that can be unlearned with consistent behavioral change. When sleep onset arrives, move to the bed. Do not try to force sleep from a state of wakefulness in a stimulating environment.
-
Regular sleep and wake times — even on weekends. Social jet lag — the disruption caused by variable weekend schedules — is a documented suppressor of slow-wave sleep quality during the week.
Search “sleep hygiene” and begin incorporating these changes systematically. Each one produces measurable improvement in slow-wave sleep architecture — and each increment of improvement in slow-wave sleep is an increment of improvement in glymphatic clearance.
Step 2: Lateral Sleep Position
-
Published data shows that lateral sleep position — either left or right side — produces greater glymphatic clearance than supine (back) or prone (stomach) sleeping5
-
Left lateral is preferred for patients with concurrent LPR or posterior sinonasal disease — it reduces nocturnal acid reflux simultaneously
-
A body pillow or positional wedge can help maintain lateral position through the night for patients who naturally return to supine sleeping
-
Head elevation of 10–15 degrees also supports both glymphatic drainage and LPR reduction simultaneously
Step 3: Hydration — Filling the Glymphatic Tank
-
Cerebrospinal fluid is approximately 99% water. Glymphatic flow — the movement of CSF through the perivascular channels — is directly dependent on adequate CSF volume. Chronic dehydration reduces CSF production and impairs glymphatic flow before the patient notices any other sign of fluid deficit.
-
The body prioritizes fluid distribution — blood volume first, organ perfusion second, cerebrospinal fluid third. By the time a chronically dehydrated patient feels thirsty, their CSF compartment has already been rationed.
-
Drink consistently throughout the day — not a large bolus at night. Evening fluid loading increases nocturnal voiding, which fragments sleep and directly impairs the slow-wave sleep that glymphatic clearance depends on.
-
Personalized target: body weight in pounds divided by two, in ounces — adjusted upward for Arizona climate, exercise, and medication burden
-
Pale yellow urine throughout the day is your most reliable real-time indicator of adequate hydration
Step 4: Movement — Activating the Whole System
-
Physical movement activates the peripheral lymphatic system — the downstream recipient of glymphatic output. A sluggish peripheral lymphatic system creates back-pressure that impairs the meningeal lymphatic drainage of glymphatic waste. Keeping the peripheral system moving keeps the central drain open.
-
Toe bounce at the bathroom sink — morning and evening — two minutes — the most efficient whole-body lymphatic pump available without equipment
-
Head and neck self-massage — three minutes — following the cervical lymph node chain downward toward the clavicle — directly activates the nodes that receive glymphatic output
-
Hot shower before sleep — heat dilates lymphatic vessels, activates glymphatic flow, and reduces the peripheral vascular resistance that supports lymphatic clearance
-
Avoid prolonged sedentary periods during the day — the cervical lymphatic congestion that develops during eight to ten hours of sitting directly impairs the lymphatic network that drains the glymphatic system’s output at night
Step 5: Nasal Airway Restoration
-
This is the highest-yield single intervention for glymphatic optimization in patients with nasal obstruction — and it is the intervention that most patients never connect to their cognitive symptoms
-
In-office options at SAWC: turbinate reduction (radiofrequency RhinAir, NEUROMARK®, or submucosal), swell body reduction, nasal valve repair (Vivaer), balloon sinuplasty for patients with sinus drainage obstruction
-
The goal: reduce nasal airway resistance sufficiently to allow normal nasal breathing during sleep — the prerequisite for sustained slow-wave sleep and optimal glymphatic clearance
-
Short of a formal surgical procedure, nasal breathing improvement can begin immediately with: daily holistic nasal rinse (xylitol + JBS 1% + Manuka honey UMF 16+), topical nasal steroid spray (fluticasone, budesonide), nasal dilator strips at night, and treatment of the upstream inflammatory drivers (allergy, LPR)
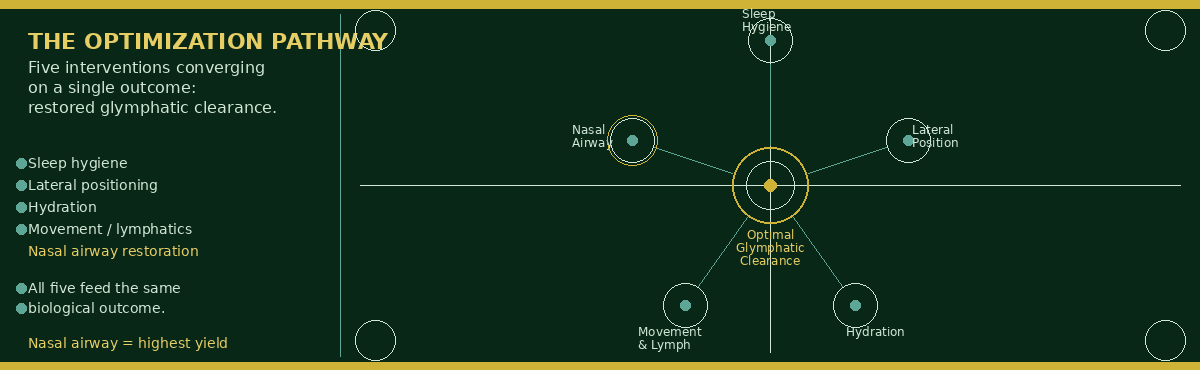
The diagram below maps the complete glymphatic optimization pathway — from behavioral interventions through nasal airway restoration — showing how each step in the protocol contributes to restoring slow-wave sleep and maximizing overnight brain clearance.
What Patients Actually Experience When This Works
When all of these elements are incorporated into a consistent daily routine, what the patient experiences is homeostasis — the glymphatic tissues processing the brain’s inflammatory content with enough efficiency that the immune system can stay ahead of what it is being asked to clear. The improvements are noticed quickly and reliably.
The brain fog lifts — not all at once, but progressively over the first two to four weeks as the accumulated neuroinflammatory burden begins to clear. Word retrieval becomes faster. Concentration extends. The mid-afternoon cognitive wall that the patient had accepted as normal begins to move and then disappear. Morning fatigue — the exhaustion that greets the patient before the day has started — diminishes as slow-wave sleep quality improves and the cleaning cycle completes.
These improvements are not side effects of sinus treatment. They are the direct consequence of restoring the brain’s primary nocturnal maintenance system. They are what happens when the glymphatic system is finally given the conditions it needs to do the job it was designed to do.
Dr. G’s Clinical Pearls
-
The glymphatic system was hidden from science until 2013 because the brain has no obvious lymphatic channels or nodes. What it has instead is a network of perivascular spaces managed by astrocyte cells — and a functional connection to the peripheral lymphatic system through the meningeal lymphatics that nobody had documented before Nedergaard’s team showed it. The discovery changes everything about how we think about sleep, neurodegeneration, and the cognitive consequences of chronic nasal obstruction.
-
Slow-wave sleep is not just rest. It is the biological state in which the brain’s interstitial space expands by up to 60 percent and glymphatic flow increases by a factor of two or more. Every hour of fragmented sleep — every hour spent in light sleep rather than deep slow-wave sleep because of nasal obstruction — is an hour of reduced brain clearance. The debt accumulates.
-
Amyloid beta and tau — the proteins of Alzheimer’s disease — are cleared by the glymphatic system during sleep. A patient with chronic nasal obstruction who has been sleeping poorly for five years has been accumulating these proteins at a rate their brain cannot clear. For a patient with a family history of Alzheimer’s, this is not an abstract concern. It is a direct biological risk that can be addressed by treating the nasal obstruction that is fragmenting their sleep.
-
Lateral sleep position produces measurably greater glymphatic clearance than supine or prone sleeping. This is the simplest zero-cost intervention available. Every patient with brain fog, morning fatigue, or a family history of dementia should be sleeping on their side. Left lateral is preferred — it simultaneously reduces nocturnal LPR events in patients with posterior sinonasal disease.
-
Dehydration reduces CSF production before the patient feels thirsty. The glymphatic system cannot move fluid it does not have. Hydration is not supportive care in the context of glymphatic optimization — it is a direct intervention on the volume of fluid available for brain clearance. Most of my brain-fog patients are chronically underhydrated and have no idea.
-
The PSS hypothesis — pepsin from silent reflux depositing on the posterior sinonasal mucosa and driving chronic inflammation — has a potentially unexplored connection to glymphatic function. The meningeal lymphatics exit the skull in anatomical proximity to the posterior nasal cavity. Whether chronic posterior sinonasal inflammation impairs these drainage pathways is a hypothesis worth testing. I propose it here as a direction for future investigation.
-
Pepsin is now confirmed as a carcinogen in the upper airway — linked to laryngeal and nasopharyngeal cancer. I propose that as the research expands, its role in other head and neck cancers will be established. Posterior sinonasal disease in a patient with confirmed LPR and pepsin exposure is not merely a quality-of-life condition. It may be a pre-malignant one. Treat it with that urgency.
-
When a patient comes back after their nasal procedure and tells me they had no idea sleep could feel the way it now feels — that is not a testimonial about their sinuses. That is a report from their glymphatic system that it has been restored to function. The most important thing I can tell that patient is: protect this. The habits that optimize glymphatic clearance are not a post-procedure protocol. They are a lifelong practice.
References
-
Nedergaard M. Garbage truck of the brain. Science. 2013;340(6140):1529-1530. doi:10.1126/science.1240514
-
Iliff JJ, Wang M, Liao Y, et al. A paravascular pathway facilitates CSF flow through the brain parenchyma and the clearance of interstitial solutes, including amyloid β. Sci Transl Med. 2012;4(147):147ra111. doi:10.1126/scitranslmed.3003748
-
Louveau A, Smirnov I, Keyes TJ, et al. Structural and functional features of central nervous system lymphatic vessels. Nature. 2015;523(7560):337-341. doi:10.1038/nature14432
-
Kress BT, Iliff JJ, Xia M, et al. Impairment of paravascular clearance pathways in the aging brain. Ann Neurol. 2014;76(6):845-861. doi:10.1002/ana.24271
-
Lee H, Xie L, Yu M, et al. The effect of body posture on brain glymphatic transport. J Neurosci. 2019;39(13):2414-2423. doi:10.1523/JNEUROSCI.2914-18.2019
-
Aspelund A, Antila S, Proulx ST, et al. A dural lymphatic vascular system that drains brain interstitial fluid and macromolecules. J Exp Med. 2015;212(7):991-999. doi:10.1084/jem.20142290
-
Johnston M, Zakharov A, Papaiconomou C, Salmasi G, Armstrong D. Evidence of connections between cerebrospinal fluid and nasal lymphatic vessels in humans, non-human primates and other mammalian species. Cerebrospinal Fluid Res. 2004;1(1):2. doi:10.1186/1743-8454-1-2
-
Gergits FR. The Sinus Is the Victim, Pepsin Is the Perpetrator: Posterior Sinonasal Syndrome as a Driver of Chronic Rhinosinusitis. Preprints. 2026. doi:10.20944/preprints202603.0858.v1
-
Wassenaar E, Johnston N, Merati A, et al. Pepsin detection in patients with laryngopharyngeal reflux before and after fundoplication. Surg Endosc. 2011;25(12):3870-3876. doi:10.1007/s00464-011-1813-1
-
Patel DA, Blanco M, Vaezi MF. Laryngopharyngeal reflux and esophageal disease. Gastrointest Endosc Clin N Am. 2014;24(1):15-27. doi:10.1016/j.giec.2013.08.003
Want to Understand More?
This article is published in the Journal of Airway Inflammation section of the Airway & Sinus Wellness Review.
→ Breaking the Biofilm: The Holistic Sinus Rinse Protocol
→ Before You Fill That Antibiotic Prescription, Try This First
→ Can Sinus Infections Cause Brain Fog — or Even Look Like Dementia?
→ Browse the full Airway & Sinus Wellness Review
Journal of Airway Inflammation — Clinical science from the Sinus & Allergy Wellness Center of North Scottsdale.
About the Author
Franklyn R. Gergits, DO, MBA, FAOCO is an otolaryngologist and rhinologist with over 30 years of clinical experience. He is the founder of the Sinus & Allergy Wellness Center of North Scottsdale, where he performs in-office balloon sinuplasty, turbinate reduction, NEUROMARK®, and swell body reduction under local anesthesia. He performed the first balloon sinuplasty in Pennsylvania, holds dual Entellus Centers of Excellence certifications, and is the originator of the Posterior Sinonasal Syndrome (PSS) hypothesis, with a preprint available at Preprints.org (DOI: 10.20944/preprints202603.0858.v1). ORCID: 0009-0000-4893-6332.
SinusAndAllergyWellnessCenter.com · 480-525-8999
This content is for educational purposes and clinical discussion purposes. It represents the author’s clinical observations and hypotheses and should not be interpreted as established medical consensus where noted as hypothetical. Consult a qualified physician for individualized evaluation and treatment recommendations.
Disclaimer:
The information provided in this article is for informational and educational purposes only and does not constitute medical advice. It is not intended to diagnose, treat, cure, or prevent any disease or medical condition. Always seek the guidance of your physician or other qualified healthcare provider with any questions you may have regarding a medical condition or treatment.
Results may vary: Treatment outcomes and health experiences may differ based on individual medical history, condition severity, and response to care.
Emergency Notice: If you are experiencing a medical emergency, call 911 or seek immediate medical attention.
