When the Airway Is the Answer — Not Just the Address

I do not look at the nose, sinuses, throat, or sleep as separate problems. I look at them as parts of one connected system. That may sound straightforward, but in practice it represents a fundamentally different way of approaching a patient — one that leads to more complete evaluations, more individualized treatment plans, and outcomes that hold rather than revolve.
Most sinus and allergy patients who arrive at my practice have already been treated. They have had antibiotics. Some have had surgery. Many have been told their imaging looks normal. And yet they are still symptomatic — still congested, still draining, still fatigued, still frustrated. What they have almost universally not had is a clinician who looked at the airway as a whole and asked: what is disrupting this system, and why?
That question is where this framework begins.
Clinical answers written in plain language — not marketing. Subscribe to the Airway & Sinus Wellness Review.
The Airway Is One System — Not Six Separate Problems
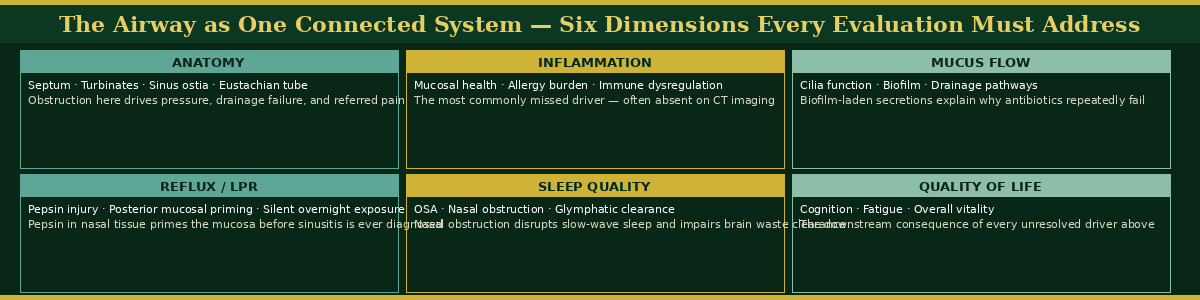
When a patient comes to me with chronic sinusitis, I am not only thinking about the sinuses. I am thinking about the nasal anatomy that governs drainage. I am thinking about the allergy burden that is driving mucosal inflammation. I am thinking about mucus flow and whether biofilm has altered the microbial environment. I am thinking about reflux — specifically laryngopharyngeal reflux — and whether pepsin is quietly injuring the posterior nasal mucosa overnight while the patient sleeps.1,2
I am thinking about sleep quality, because nasal obstruction disrupts slow-wave sleep, and disrupted sleep impairs glymphatic clearance, and that cascade connects airway disease to cognitive symptoms in ways that most patients have never been told.3 And I am thinking about quality of life — not as an afterthought, but as a clinical variable that tells me how far the disease has progressed and how urgently the system needs to be reset.
Instead of asking only “what symptom does this patient have,” the right question is “what is disrupting the airway overall.” That shift — from symptom to system — is what produces a complete evaluation and a treatment plan that addresses the actual driver rather than the most visible complaint.4
“The framework below maps the six dimensions of airway evaluation that inform every clinical encounter at SAWC — and the clinical significance of each. Disruption in any one of these areas can drive symptoms that appear to originate somewhere else entirely.”
Patient Education Is Not Optional — It Is the Intervention
One of the most important shifts in my practice over thirty years has been the central role of patient education — not as a courtesy, and not merely as informed consent, but as a therapeutic intervention in its own right.
When patients can actually see what is happening — when they watch their own nasal endoscopy in real time, when they look at their CT scan with someone who explains what they are seeing rather than simply reading them a report — something changes. The fear that has been sustaining their anxiety about their symptoms is replaced by something more productive: direction. A patient who understands their condition makes better decisions, follows through on treatment, and does not require repeated re-education at every visit.
My goal has never been to push a procedure. My goal is to help the patient understand what we found, what the likely drivers are, what conservative care can realistically accomplish, and when a procedure offers a genuinely better path. An informed patient is a more comfortable patient, a more committed patient, and ultimately a more successful one.5 The moment they see an objective clinical reason for their discomfort — on the scope, on the scan — their fear is replaced by a sense of direction and partnership. That shift costs nothing except the time to explain it properly.
How Minimally Invasive Techniques Changed the Conversation
Balloon sinuplasty helped move sinus care toward a more physiologic, tissue-preserving, and patient-friendly approach.6 It changed the conversation in the specialty from “how much tissue do we remove” to “how can we restore drainage and function as gently as possible.” That was an important and necessary shift.
It also made it possible for properly selected patients to be treated in the office setting — under local anesthesia, without general anesthesia, without hospital admission — with less disruption, faster recovery, and less need for more invasive surgery. I performed the first balloon sinuplasty in Pennsylvania. In the years since, I have watched the technology evolve, the evidence base deepen, and the patient experience improve as protocols have been refined.
But the most important change balloon sinuplasty produced was not procedural. It was philosophical. It pushed the entire field to think more carefully about function, recovery, and patient experience — and that philosophical shift made room for the broader airway-focused framework that now guides everything we do at SAWC.
Innovation Responsibly Applied
Being part of the early advancement of balloon sinuplasty also taught me something that has stayed with me through every subsequent innovation I have encountered or adopted: new technology is only valuable when it is matched to the right patient for the right reason.
Innovation should improve care, not simply make care newer. That means understanding the anatomy, the disease process, the limitations of the tool, and the long-term outcome you are trying to achieve before you reach for any new instrument. It means staying excited about progress while remaining disciplined enough to ask — at every patient encounter — whether this intervention is truly best for this specific person.
Technology is a tool, not a philosophy. The fundamentals still matter most: listening carefully, examining thoroughly, identifying the true driver of disease, and choosing the least disruptive treatment that gives the patient the best chance of meaningful improvement.7 When new technology genuinely supports those principles, it can be extraordinarily powerful. When it distracts from them, it should not lead the decision.
A Comprehensive Evaluation Versus a Symptom-Only Approach
A symptom-only approach reacts to what the patient feels in the moment. A comprehensive ENT evaluation tries to understand why that symptom is happening — and what system is producing it.
That distinction matters enormously in practice. Facial pressure does not always mean sinusitis. Ear pressure does not always mean ear disease. Throat symptoms may not begin in the throat. Post-nasal drainage that fails every treatment may be driven by a posterior nerve that is overactive, not by a sinus that is infected. The symptom and its source are frequently not the same location — and treating the location rather than the source is exactly what produces the revolving door of temporary relief followed by return of symptoms that so many chronic patients know by heart.8
A comprehensive evaluation connects the symptom to the system behind it. It includes a careful history, nasal endoscopy, imaging when appropriate, allergy consideration, airway function assessment, and an honest conversation about the relationship between anatomy and inflammation. It does not rush to the most obvious explanation. It does not anchor prematurely on the presenting complaint. And it does not end with a prescription — it ends with a plan.
Balancing New Technology With Proven Clinical Principles
I always start with proven clinical principles and then ask whether technology adds meaningful value for this patient. Careful listening. Thorough examination. Honest identification of the true driver of disease. The least disruptive treatment that gives the patient the best chance of improvement. These fundamentals do not change — and no technology replaces them.
What NEUROMARK® (Neurent Medical, FDA-cleared radiofrequency ablation system targeting the posterior nasal nerve) adds to the balloon sinuplasty framework is the ability to address the neurological driver of chronic drainage and congestion that persists even when anatomy has been corrected and inflammation has been managed.9 When the system is overreactive — when the posterior nerve has been sensitized by months or years of mucosal inflammation, reflux injury, and allergy priming — down-regulating that overactive signaling produces relief that structural correction alone cannot achieve.
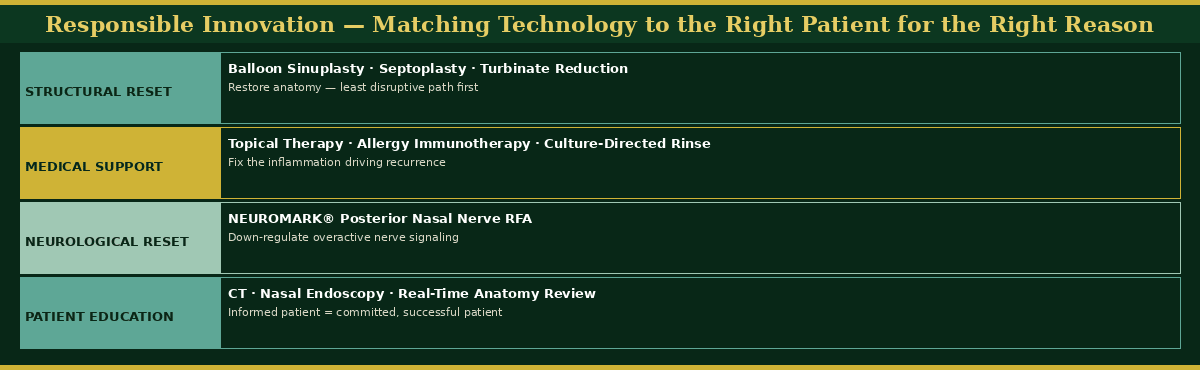
By combining a structural reset with medical support and a neurological reset, we stop the revolving door of chronic symptoms and provide a lasting solution — not because we did more, but because we identified every driver and addressed each one in the right sequence.
“The framework below illustrates the layered treatment approach at SAWC — structural reset, medical support, neurological reset, and patient education — and what each layer is designed to accomplish. The sequence matters: procedures follow conservative care, not replace it.”
Dr. G’s Clinical Pearls
Pearl 1
Showing a patient their own nasal endoscopy in real time is one of the most therapeutically significant moments in the entire clinical encounter. The pain that was invisible and inexplicable becomes visible and explicable. The patient who felt unseen becomes a patient with a map. Never underestimate the healing power of a visible plan.
Pearl 2
Innovation is only valuable when matched to the right patient for the right reason. New technology should never replace good clinical judgment — it should sharpen it. The question at every encounter is not “what is the newest tool available” but “what does this specific patient actually need.”
Pearl 3
The patients who make the most meaningful and lasting progress are the ones who had three things: a clear diagnosis grounded in objective data, the ability to see that data with their own eyes, and a sequential treatment plan with a defined next step at every stage. Control comes from clarity and direction — not from procedures alone.
Pearl 4
Good ENT care is not about doing more — it is about doing what is right for the patient. The best clinical outcomes in thirty years of rhinologic practice have not come from the most aggressive interventions. They have come from the most precise ones: the right treatment, matched to the right driver, delivered at the right time.
References
-
Yadav M, Coumar MS. Pepsin and laryngopharyngeal reflux: a comprehensive review. World J Gastroenterol. 2023;29(6):968-985.
-
Gergits FR. The Sinus Is the Victim, Pepsin Is the Perpetrator: Posterior Sinonasal Syndrome as the Etiological Precursor to Chronic Rhinosinusitis. Preprints. 2026. doi:10.20944/preprints202603.0858.v1
-
Xie L, Kang H, Xu Q, et al. Sleep drives metabolite clearance from the adult brain. Science. 2013;342(6156):373-377.
-
Fokkens WJ, Lund VJ, Hopkins C, et al. European Position Paper on Rhinosinusitis and Nasal Polyps 2020. Rhinology. 2020;58(Suppl S29):1-464.
-
Mularski RA, Asch SM, Shrank WH, et al. The quality of obstructive sleep apnea management in community-based physician practices. Sleep. 2006;29(10):1306-1311.
-
Gould J, Alexander I, Tomkin E, Brodner D. In-office, multisinus balloon dilation: 1-year outcomes from a prospective, multicenter, open-label trial. Am J Rhinol Allergy. 2014;28(2):156-163.
-
Rosenfeld RM, Piccirillo JF, Chandrasekhar SS, et al. Clinical Practice Guideline (Update): Adult Sinusitis. Otolaryngol Head Neck Surg. 2015;152(2 Suppl):S1-S39.
-
Meltzer EO, Hamilos DL. Rhinosinusitis diagnosis and management for the clinician: a synopsis of recent consensus guidelines. Mayo Clin Proc. 2011;86(5):427-443.
-
Shaari CM, Sanders I, Wu BL, Biller HF. Rhinorrhea is decreased in dogs after nasal application of botulinum toxin. Otolaryngol Head Neck Surg. 1995;112(5):566-571.
Want to Understand More?
This post is part of the Journal of Airway Inflammation on the Airway & Sinus Wellness Review.
FAQ: Why Antibiotics Keep Failing Your Sinus Infection
FAQ: Does Balloon Sinuplasty Actually Work?
FAQ: Will Balloon Sinuplasty Correct My Post-Nasal Drainage?
The Final Chapter: What the Field Still Cannot See — Posterior Sinonasal Syndrome
Journal of Airway Inflammation — Clinical education from the Sinus & Allergy Wellness Center of North Scottsdale.
About the Author
Franklyn R. Gergits, DO, MBA, FAOCO is an otolaryngologist and rhinologist with over 30 years of clinical experience treating sinus and airway disease. He is the founder of the Sinus & Allergy Wellness Center of North Scottsdale and performed the first balloon sinuplasty in Pennsylvania. He holds dual Entellus Centers of Excellence certifications and specializes in office-based nasal and sinus procedures under local anesthesia, including balloon sinuplasty, turbinate reduction, NEUROMARK® posterior nasal nerve ablation (Neurent Medical, FDA-cleared radiofrequency ablation system), and Eustachian tube dilation. Dr. Gergits is the originator of the Posterior Sinonasal Syndrome (PSS) hypothesis — a clinical framework identifying posterior nasal mucosal inflammation driven by pepsin and laryngopharyngeal reflux as an etiological precursor to chronic rhinosinusitis. His manuscript is currently under peer review, with a preprint available at Preprints.org (DOI: 10.20944/preprints202603.0858.v1). ORCID: 0009-0000-4893-6332.
SinusAndAllergyWellnessCenter.com · 480-525-8999
This content is for educational purposes only and does not constitute medical advice. If you are experiencing sinus or airway symptoms, please consult a qualified physician for evaluation and individualized treatment recommendations.
Disclaimer:
The information provided in this article is for informational and educational purposes only and does not constitute medical advice. It is not intended to diagnose, treat, cure, or prevent any disease or medical condition. Always seek the guidance of your physician or other qualified healthcare provider with any questions you may have regarding a medical condition or treatment.
Results may vary: Treatment outcomes and health experiences may differ based on individual medical history, condition severity, and response to care.
Emergency Notice: If you are experiencing a medical emergency, call 911 or seek immediate medical attention.
