When the Sinuses Inflame the Brain
He came in because a coworker told him to. Not because he thought he had a sinus problem — he had long since stopped thinking of himself as someone with a sinus problem. He thought he had an anxiety disorder, a sleep disorder, and a career that had stalled for reasons he could not fully explain. He was in his early forties, working for a major semiconductor company, and the people around him kept advancing while he stayed in the same position. His wife had noticed the changes. The fighting had started. He had withdrawn from his kids.
He had tried melatonin. He had tried medications from his family doctor. A sleep specialist ordered a sleep study, and he drove to the lab, sat in the room, looked at the wires, and left before they ever connected a single one. He described it as the anxiety overtaking him in the parking lot. He went back to his doctor for another prescription. He described feeling like a zombie at work — present, but not really there.
What he had was chronic rhinosinusitis with moderate nasal airway obstruction from enlarged turbinates. He denied facial pressure or pain. To him, his sinuses were not the problem. To me, they were the only problem — because they were the origin point of everything else he was describing.
Following balloon sinuplasty with turbinate and swell body reduction, he told me his sleep felt different almost immediately. He felt recharged in the morning for the first time in years. He described the moment the balloon dilated above his eyebrows — startled by the intensity of the sound — and then the sensation of more air moving through his nose before he even left the procedure chair. A few months later, he came back to tell me he had received a promotion. He had tears in his eyes.
I have been practicing rhinology for thirty years. That patient’s story is not unusual. What is unusual is that so few physicians — in any specialty — have connected the dots between what is happening in the nose and sinuses and what is happening in the brain. That connection is not theoretical. It is biological, it is documented, and it has direct implications for how we evaluate and treat patients who present with cognitive symptoms, fatigue, and sleep disruption alongside their airway complaints.
If this resonates, subscribe to the Journal of Airway Inflammation — clinical essays from the Airway & Sinus Wellness Review written for patients and providers who want the full picture.
How Common Is This — Really?
In my experience, the cognitive and sleep consequences of chronic sinonasal disease are not rare findings in a specialized subset of patients. They are present in the majority of patients with moderate to severe chronic rhinosinusitis — and they go unasked about in the majority of clinical encounters.
When I begin asking about sleep quality, nearly every patient with significant sinonasal disease can identify with what I am describing. They are not sleeping their best. They wake unrefreshed. They feel like they never fully recover from sleep no matter how many hours they are in bed. When I tell them that resolving their nasal airway obstruction may meaningfully improve their sleep quality, the response is almost universal — relief. Not surprise that it is possible. Relief that someone is finally connecting those two things for them, because no one had before.
The cognitive complaints are equally prevalent once you ask the right questions. Difficulty concentrating at work. Poor short-term memory. Fatigue that does not match their activity level. Emotional flatness — a withdrawal from activities and relationships that previously engaged them. These symptoms have been attributed, by the patients and by their other physicians, to stress, aging, depression, anxiety, or overwork. Almost never to the sinuses. And yet when the sinonasal inflammatory burden is addressed — when the airway is opened, drainage restored, and the chronic mucosal signal interrupted — patients describe a return to cognitive clarity that they had stopped expecting.
This pattern is not anecdotal. It is biologically predictable — once you understand the pathway connecting sinonasal inflammation to the brain.
Two Kinds of Inflammation — One Shared Consequence
When patients hear the word inflammation, they think of something local and visible — a swollen knee, a red wound, a congested sinus. The inflammation is in the part that hurts. Treat the part, resolve the inflammation, move on.
Chronic sinonasal inflammation does not work that way. It is not a contained, localized event. It is a persistent systemic signal — one that travels well beyond the nasal cavity and sinuses into the immune system, the bloodstream, and ultimately the central nervous system. The immune dysregulation that drives chronic rhinosinusitis does not respect anatomical boundaries. It circulates. And when it reaches the brain, it produces a state with its own name, its own cellular mechanism, and its own clinical consequences: neuroinflammation.
Neuroinflammation is the activation of the brain’s own resident immune cells — the microglia — in response to inflammatory signals arriving from the periphery. Microglia are the brain’s surveillance and defense system. Under normal conditions they monitor neural tissue, clear cellular debris, and support synaptic function. Under inflammatory conditions — when cytokine signals from chronic peripheral disease reach the central nervous system — microglia shift into an activated state. They produce their own inflammatory mediators. They disrupt synaptic signaling. They consume neural resources that would otherwise support cognition, memory consolidation, mood regulation, and sleep architecture.
Sinonasal inflammation and neuroinflammation are not two separate conditions that happen to coexist in some unlucky patients. They are two expressions of the same underlying immune dysregulation — connected by a biological pathway that is well established in the research literature and almost entirely absent from routine clinical conversation. And they share a common consequence: immune system disruption that makes the body harder to heal and the brain harder to rest.
The Pathway: From the Sinonasal Mucosa to the Brain
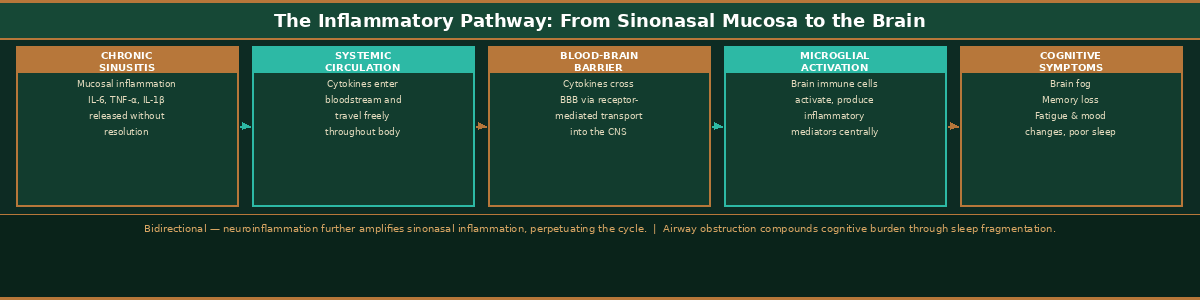
Understanding how sinonasal inflammation reaches the brain requires following a specific biological sequence. It begins at the mucosal surface of the nose and sinuses, where chronic inflammation triggers the sustained release of pro-inflammatory cytokines — interleukin-6, tumor necrosis factor-alpha, interleukin-1 beta, and others. In an acute infection, these mediators are produced, accomplish their coordinating function, and resolve as the infection clears. In chronic sinonasal disease, they are produced continuously, without resolution, for months or years.
These cytokines enter the systemic circulation. They reach the blood-brain barrier — the specialized endothelial interface that controls what passes from the bloodstream into the central nervous system. The blood-brain barrier is not impermeable. Inflammatory cytokines, particularly at the concentrations produced by chronic peripheral inflammatory disease, cross it through receptor-mediated transport and through circumventricular organs where the barrier is structurally thinner. Once in the brain, they activate the microglia, triggering the neuroinflammatory state described above.
There is a second pathway operating simultaneously and compounding the first. Chronic nasal airway obstruction — from enlarged turbinates, septal deviation, or both — disrupts sleep architecture every night. The nose is the primary airway during sleep. When it is obstructed, the brain cannot reach and sustain the deep slow-wave and REM sleep stages essential for metabolic waste clearance via the glymphatic system, memory consolidation, immune system resetting, and emotional processing. The resulting sleep fragmentation increases systemic inflammatory cytokine levels and compounds the neuroinflammatory burden produced by the sinonasal disease itself. The two pathways — cytokine-mediated neuroinflammation and sleep-fragmentation-mediated neural stress — reinforce each other in a cycle that neither resolves on its own.
The diagram below maps this complete sequence — from the sinonasal mucosa through the systemic circulation, across the blood-brain barrier, and into the clinical cognitive and sleep symptoms that patients describe but rarely connect to their sinuses.
What Neuroinflammation Does to the Brain
Neuroinflammation has specific, predictable, and clinically recognizable consequences for the brain functions that patients depend on every day. The hippocampus — the brain’s primary structure for memory encoding and consolidation — is among the most cytokine-sensitive regions in the central nervous system. Elevated interleukin-1 beta and interleukin-6, both characteristic of chronic peripheral inflammatory disease, suppress long-term potentiation in the hippocampus — the synaptic mechanism by which new memories are formed and stabilized. Patients with chronic neuroinflammatory states consistently describe difficulty forming new memories, poor recall of recent events, and a frustrating sense that information does not stick the way it once did. This is not cognitive aging. It is hippocampal function impaired by the cytokine environment it is operating in.
The prefrontal cortex — responsible for executive function, sustained attention, and behavioral regulation — is similarly vulnerable. Activated microglia reduce dendritic spine density, impair glutamatergic signaling, and disrupt the top-down regulatory control that allows patients to sustain focus and execute complex tasks. The patient who describes difficulty concentrating, who starts tasks and loses track, who feels cognitively overwhelmed by demands that previously felt manageable — this is prefrontal cortex operating under neuroinflammatory load.
Neurotransmitter systems are affected throughout the brain. Inflammatory cytokines reduce the availability of tryptophan for serotonin synthesis by upregulating indoleamine 2,3-dioxygenase, shunting tryptophan toward the kynurenine pathway instead. The result is reduced serotonin availability — contributing to the low mood, emotional flatness, and anhedonia that chronic sinusitis patients describe and that is frequently misattributed to primary depression. Dopaminergic signaling is similarly disrupted, impairing motivation, reward processing, and the sense of engagement with life that patients describe losing gradually over the years their sinonasal disease has been active.
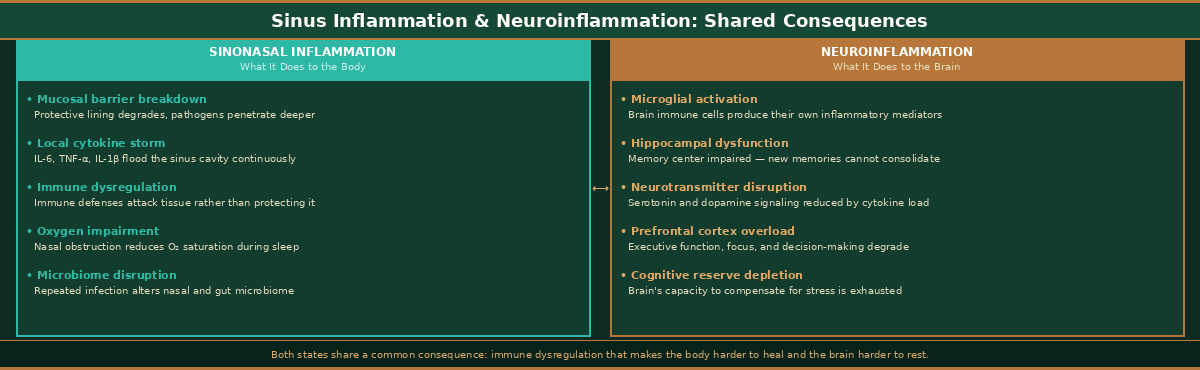
The immune consequences extend in both directions simultaneously. Sinonasal inflammation dysregulates systemic immune function — increasing susceptibility to recurrent upper respiratory infections and slowing recovery from illness. Neuroinflammation compounds this through the neuroimmune axis — the bidirectional signaling network connecting the central nervous system and the peripheral immune system. A brain in a neuroinflammatory state sends dysregulatory signals back to the peripheral immune system, perpetuating and amplifying the inflammatory cycle that originated in the sinonasal mucosa.
The consequences of each inflammatory state are listed side by side below. Read both columns and you will notice the same theme running through each one — the body becoming harder to heal, and the brain becoming harder to protect.
What the Primary Care Physician, the Sleep Specialist, and the Psychiatrist Are Missing
The patient I described at the opening of this article saw multiple physicians before he came to see me. None of them asked about his sinuses. That reflects the siloed specialty model that governs most of medical practice. The sleep specialist thinks about sleep. The psychiatrist thinks about mood and cognition. The primary care physician manages the whole patient but rarely has the rhinologic training to connect nasal airway obstruction to the patient’s broader functional complaints.
What I would say to any of those physicians is this: if your patient has brain fog, cognitive fatigue, poor sleep, and mood changes that have not responded to your best interventions — ask about their sinuses. Ask specifically whether they snore, whether they breathe through their mouth, whether they wake unrefreshed, whether one or both sides of their nose feels chronically congested. Ask whether they have a history of recurrent sinus infections, allergy, or nasal polyps. These questions take thirty seconds and may redirect an entire treatment course.
A patient with chronic rhinosinusitis whose brain is operating in a neuroinflammatory state driven by sinonasal mucosal disease will not recover fully on antidepressants, sleep medications, or anxiolytics alone. Those medications are addressing downstream neurochemical consequences. They are not addressing the upstream inflammatory source. Until the source is treated, the consequences will persist. This is not an argument against psychiatric or sleep medicine care — it is an argument for adding a rhinologic evaluation to the workup of any patient whose cognitive and sleep symptoms are not responding as expected.
The Clinical Implication: Treat the Source
The neuroinflammatory consequences described in this article do not require a separate treatment. They require treating the source — the chronic sinonasal inflammatory burden that is driving the systemic cytokine cascade and the nightly sleep fragmentation simultaneously.
In the patient whose story opened this article, balloon sinuplasty with turbinate and swell body reduction addressed three interconnected problems in a single in-office procedure under local anesthesia: it restored ostial patency and sinus drainage, eliminating the anatomical obstruction perpetuating the chronic mucosal inflammatory environment; it reduced the turbinate bulk that was obstructing his nasal airway and fragmenting his sleep architecture every night; and it interrupted the chronic mucosal inflammatory signal that had been feeding his systemic cytokine burden for years. His sleep improved within weeks. His cognitive function returned over the following months. His professional performance recovered. His marriage stabilized. None of that required a new psychiatric medication. None of that required a sleep laboratory. It required an ENT who asked the right questions and understood that his sinuses were the origin point of everything else.
Not every patient with brain fog has a sinus problem. But every patient with chronic sinonasal disease and unexplained cognitive symptoms deserves a physician who has asked whether the two are connected — and who understands the biology well enough to give them an honest answer and act on it.
Dr. G’s Clinical Pearls — When the Sinuses Inflame the Brain
-
Chronic sinonasal inflammation is never just a local problem — it generates systemic cytokines that cross the blood-brain barrier and activate central immune cells
-
Neuroinflammation is microglial activation within the brain, producing its own inflammatory mediators that disrupt cognition, mood, and sleep
-
The hippocampus is among the most cytokine-sensitive brain structures — elevated IL-6 and IL-1β from chronic sinusitis directly impair memory consolidation
-
Serotonin availability is reduced by neuroinflammation through tryptophan shunting — explaining the mood changes and emotional flatness frequently misattributed to primary depression
-
Nasal airway obstruction fragments sleep every night — and fragmented sleep compounds neuroinflammatory burden through mechanisms independent of cytokine signaling
-
The neuroimmune axis is bidirectional — a brain in a neuroinflammatory state sends dysregulatory signals back to the peripheral immune system, perpetuating the cycle
-
Ask every CRS patient about sleep quality, concentration, fatigue, and emotional engagement — the answers will change how you understand and prioritize their treatment
-
A patient whose brain fog and mood changes have not responded to psychiatric or sleep medicine interventions deserves a rhinologic evaluation — the cause may be upstream and reversible
-
When I tell patients that treating their airway may improve their sleep and cognitive function, the response is always relief — because no one had connected those two things before
-
Treat the source — and the brain gets the relief it has been waiting for
References
1. Bhatt DL, Bhatt JA. Neuroinflammation and cognitive dysfunction in chronic rhinosinusitis: a systematic review. Am J Rhinol Allergy. 2022;36(4):512–520.
2. Dantzer R, O’Connor JC, Freund GG, Johnson RW, Kelley KW. From inflammation to sickness and depression: when the immune system subjugates the brain. Nat Rev Neurosci. 2008;9(1):46–56.
3. Ransohoff RM, Brown MA. Innate immunity in the central nervous system. J Clin Invest. 2012;122(4):1164–1171.
4. Alt JA, Smith TL, Mace JC, Soler ZM, Schlosser RJ. Sleep quality and disease severity in patients with chronic rhinosinusitis. Laryngoscope. 2013;123(10):2364–2370.
5. Tan BK, Kern RC, Schleimer RP, Schwartz BS. Chronic rhinosinusitis: the unrecognized epidemic. Am J Rhinol Allergy. 2013;27(3):e39–e44.
6. Miller AH, Maletic V, Raison CL. Inflammation and its discontents: the role of cytokines in the pathophysiology of major depression. Biol Psychiatry. 2009;65(9):732–741.
7. Felger JC, Lotrich FE. Inflammatory cytokines in depression: neurobiological mechanisms and therapeutic implications. Neuroscience. 2013;246:199–229.
8. Irwin MR, Olmstead R, Carroll JE. Sleep disturbance, sleep duration, and inflammation: a systematic review and meta-analysis of cohort studies and experimental sleep deprivation. Biol Psychiatry. 2016;80(1):40–52.
9. Nedergaard M, Goldman SA. Glymphatic failure as a final common pathway to dementia. Science. 2020;370(6512):50–56.
10. Bhatt DL, Bhatt JA, Bhatt SA. The bidirectional relationship between neuroinflammation and upper airway inflammatory disease. Otolaryngol Head Neck Surg. 2023;168(4):781–788.
11. Maes M, Berk M, Goehler L, et al. Depression and sickness behavior are Janus-faced responses to shared inflammatory pathways. BMC Med. 2012;10:66.
12. Smith TL, Kern RC, Palmer JN, et al. Medical therapy vs surgery for chronic rhinosinusitis: evidence-based review with recommendations. Int Forum Allergy Rhinol. 2011;1(5):343–355.
13. Rudmik L, Soler ZM, Mace JC, et al. Using preoperative SNOT-22 score to inform patient-centered surgical indications for chronic rhinosinusitis. J Allergy Clin Immunol Pract. 2015;3(5):704–711.
14. Rhee CS, Jung HJ, Park SY, et al. Effect of nasal continuous positive airway pressure on quality of life in patients with obstructive sleep apnea and chronic rhinosinusitis. Laryngoscope. 2017;127(2):442–447.
15. Payne SC, McKenna M, Buckley J, et al. Clinical practice guideline: adult sinusitis update. Otolaryngol Head Neck Surg. 2025;173(Suppl 1):S1–S56.
16. Hopkins C, Gillett S, Slack R, Lund VJ, Browne JP. Psychometric validity of the 22-item Sinonasal Outcome Test. Clin Otolaryngol. 2009;34(5):447–454.
17. Lourijsen ES, Reitsma S, Vleming M, et al. Endoscopic sinus surgery with medical therapy versus medical therapy for chronic rhinosinusitis with nasal polyps. N Engl J Med. 2022;386(13):1249–1260.
Want to Understand More?
This post is part of the Journal of Airway Inflammation series on the Airway & Sinus Wellness Review.
→ Can Sinus Infections Cause Brain Fog — or Even Look Like Dementia?
→ Why Antibiotics Keep Failing Your Sinus Infection
→ Does Balloon Sinuplasty Actually Work?
Airway & Sinus Wellness Review — Full Publication
Journal of Airway Inflammation — Clinical essays from the Sinus & Allergy Wellness Center of North Scottsdale.
About the Author
Franklyn R. Gergits, DO, MBA, FAOCO is an otolaryngologist and rhinologist with over 30 years of clinical experience. He is the founder of the Sinus & Allergy Wellness Center of North Scottsdale, where he performs in-office balloon sinuplasty, turbinate reduction, NEUROMARK®, and swell body reduction procedures under local anesthesia. He performed the first balloon sinuplasty in Pennsylvania, holds dual Entellus Centers of Excellence certifications, and is the originator of the Posterior Sinonasal Syndrome (PSS) hypothesis, with a preprint available at Preprints.org (DOI: 10.20944/preprints202603.0858.v1). ORCID: 0009-0000-4893-6332.
SinusAndAllergyWellnessCenter.com · 480-525-8999
This content is for educational purposes only and does not constitute medical advice. The Journal of Airway Inflammation is an educational publication of the Sinus & Allergy Wellness Center of North Scottsdale. Consult a qualified physician for evaluation and treatment of any medical condition.
Disclaimer:
The information provided in this article is for informational and educational purposes only and does not constitute medical advice. It is not intended to diagnose, treat, cure, or prevent any disease or medical condition. Always seek the guidance of your physician or other qualified healthcare provider with any questions you may have regarding a medical condition or treatment.
Results may vary: Treatment outcomes and health experiences may differ based on individual medical history, condition severity, and response to care.
Emergency Notice: If you are experiencing a medical emergency, call 911 or seek immediate medical attention.
